

Report in English with a Dutch summary (KCE reports 45A)
Report in English with a Dutch summary (KCE reports 45A)
Report in English with a Dutch summary (KCE reports 45A)

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>KCE</strong> <strong>reports</strong> vol.45 Screen<strong>in</strong>g for Colorectal Cancer 35<br />
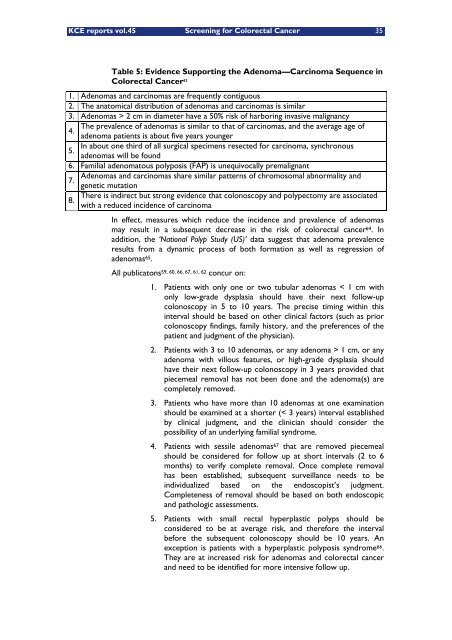
Table 5: Evidence Support<strong>in</strong>g the Adenoma Carc<strong>in</strong>oma Sequence <strong>in</strong><br />
Colorectal Cancer 63<br />
1. Adenomas and carc<strong>in</strong>omas are frequently contiguous<br />
2. The anatomical distribution of adenomas and carc<strong>in</strong>omas is similar<br />
3. Adenomas > 2 cm <strong>in</strong> diameter have a 50% risk of harbor<strong>in</strong>g <strong>in</strong>vasive malignancy<br />
The prevalence of adenomas is similar to that of carc<strong>in</strong>omas, and the average age of<br />
4.<br />
adenoma patients is about five years younger<br />
In about one third of all surgical specimens resected for carc<strong>in</strong>oma, synchronous<br />
5.<br />
adenomas will be found<br />
6. Familial adenomatous polyposis (FAP) is unequivocally premalignant<br />
Adenomas and carc<strong>in</strong>omas share similar patterns of chromosomal abnormality and<br />
7.<br />
8.<br />
genetic mutation<br />
There is <strong>in</strong>direct but strong evidence that colonoscopy and polypectomy are associated<br />
<strong>with</strong> a reduced <strong>in</strong>cidence of carc<strong>in</strong>oma<br />
In effect, measures which reduce the <strong>in</strong>cidence and prevalence of adenomas<br />
may result <strong>in</strong> a subsequent decrease <strong>in</strong> the risk of colorectal cancer 64. In<br />
addition, the National Polyp Study (US) data suggest that adenoma prevalence<br />
results from a dynamic process of both formation as well as regression of<br />
adenomas 65.<br />
All publicatons 59, 60, 66, 67, 61, 62 concur on:<br />
1. Patients <strong>with</strong> only one or two tubular adenomas < 1 cm <strong>with</strong><br />
only low-grade dysplasia should have their next follow-up<br />
colonoscopy <strong>in</strong> 5 to 10 years. The precise tim<strong>in</strong>g <strong>with</strong><strong>in</strong> this<br />
<strong>in</strong>terval should be based on other cl<strong>in</strong>ical factors (such as prior<br />
colonoscopy f<strong>in</strong>d<strong>in</strong>gs, family history, and the preferences of the<br />
patient and judgment of the physician).<br />
2. Patients <strong>with</strong> 3 to 10 adenomas, or any adenoma > 1 cm, or any<br />
adenoma <strong>with</strong> villous features, or high-grade dysplasia should<br />
have their next follow-up colonoscopy <strong>in</strong> 3 years provided that<br />
piecemeal removal has not been done and the adenoma(s) are<br />
completely removed.<br />
3. Patients who have more than 10 adenomas at one exam<strong>in</strong>ation<br />
should be exam<strong>in</strong>ed at a shorter (< 3 years) <strong>in</strong>terval established<br />
by cl<strong>in</strong>ical judgment, and the cl<strong>in</strong>ician should consider the<br />
possibility of an underly<strong>in</strong>g familial syndrome.<br />
4. Patients <strong>with</strong> sessile adenomas 67 that are removed piecemeal<br />
should be considered for follow up at short <strong>in</strong>tervals (2 to 6<br />
months) to verify complete removal. Once complete removal<br />
has been established, subsequent surveillance needs to be<br />
<strong>in</strong>dividualized based on the endoscopist s judgment.<br />
Completeness of removal should be based on both endoscopic<br />
and pathologic assessments.<br />
5. Patients <strong>with</strong> small rectal hyperplastic polyps should be<br />
considered to be at average risk, and therefore the <strong>in</strong>terval<br />
before the subsequent colonoscopy should be 10 years. An<br />
exception is patients <strong>with</strong> a hyperplastic polyposis syndrome 66.<br />
They are at <strong>in</strong>creased risk for adenomas and colorectal cancer<br />
and need to be identified for more <strong>in</strong>tensive follow up.














