

Report in English with a Dutch summary (KCE reports 45A)
Report in English with a Dutch summary (KCE reports 45A)
Report in English with a Dutch summary (KCE reports 45A)

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
184 Screen<strong>in</strong>g for Colorectal Cancer: Appendices <strong>KCE</strong> <strong>reports</strong> vol.45<br />
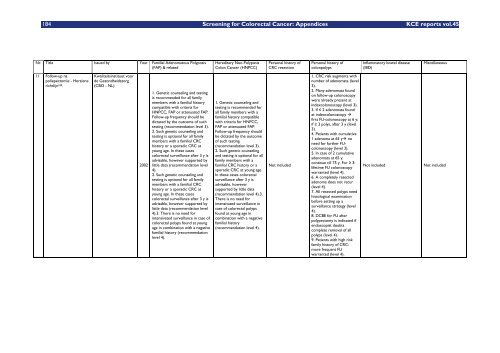
Nr. Title Issued by Year Familial Adenomatous Polyposis<br />
(FAP) & related<br />
11 Follow-up na<br />
poliepectomie - Herziene<br />
richtlijn 189.<br />
Kwaliteits<strong>in</strong>stituut voor<br />
de Gezondheidszorg<br />
(CBO - NL)<br />
2002<br />
1. Genetic counsel<strong>in</strong>g and test<strong>in</strong>g<br />
is recommended for all family<br />
members <strong>with</strong> a familial history<br />
compatible <strong>with</strong> criteria for<br />
HNPCC, FAP or attenuated FAP.<br />
Follow-up frequency should be<br />
dictated by the outcome of such<br />
test<strong>in</strong>g (recommendation level 3).<br />
2. Such genetic counsel<strong>in</strong>g and<br />
test<strong>in</strong>g is optional for all family<br />
members <strong>with</strong> a familial CRC<br />
history or a sporadic CRC at<br />
young age. In these cases<br />
colorectal surveillance after 3 y is<br />
advisable, however supported by<br />
little data (recommendation level<br />
4).<br />
2. Such genetic counsel<strong>in</strong>g and<br />
test<strong>in</strong>g is optional for all family<br />
members <strong>with</strong> a familial CRC<br />
history or a sporadic CRC at<br />
young age. In these cases<br />
colorectal surveillance after 3 y is<br />
advisable, however supported by<br />
little data (recommendation level<br />
4).3. There is no need for<br />
<strong>in</strong>tensivated surveillance <strong>in</strong> case of<br />
colorectal polyps found at young<br />
age <strong>in</strong> comb<strong>in</strong>ation <strong>with</strong> a negative<br />
familial history (recommendation<br />
level 4).<br />
Hereditary Non-Polyposis<br />
Colon Cancer (HNPCC)<br />
1. Genetic counsel<strong>in</strong>g and<br />
test<strong>in</strong>g is recommended for<br />
all family members <strong>with</strong> a<br />
familial history compatible<br />
<strong>with</strong> criteria for HNPCC,<br />
FAP or attenuated FAP.<br />
Follow-up frequency should<br />
be dictated by the outcome<br />
of such test<strong>in</strong>g<br />
(recommendation level 3).<br />
2. Such genetic counsel<strong>in</strong>g<br />
and test<strong>in</strong>g is optional for all<br />
family members <strong>with</strong> a<br />
familial CRC history or a<br />
sporadic CRC at young age.<br />
In these cases colorectal<br />
surveillance after 3 y is<br />
advisable, however<br />
supported by little data<br />
(recommendation level 4).3.<br />
There is no need for<br />
<strong>in</strong>tensivated surveillance <strong>in</strong><br />
case of colorectal polyps<br />
found at young age <strong>in</strong><br />
comb<strong>in</strong>ation <strong>with</strong> a negative<br />
familial history<br />
(recommendation level 4).<br />
Personal history of<br />
CRC resection<br />
Not <strong>in</strong>cluded<br />
Personal history of<br />
colonpolyps<br />
1. CRC risk augments <strong>with</strong><br />
number of adenomata (level<br />
3).<br />
2. Many adenomata found<br />
on follow-up colonoscopy<br />
were already present at<br />
<strong>in</strong>dexcolonoscopy (level 3).<br />
3. If 2 adenomata found<br />
at <strong>in</strong>dexcolonoscopy <br />
first FU-colonoscopy at 6 y;<br />
if 3 polys, after 3 y (level<br />
3).<br />
4. Patients <strong>with</strong> cumulative<br />
1 adenoma at 65 y no<br />
need for further FUcolonoscopy<br />
(level 3).<br />
5. In case of 2 cumulative<br />
adenomata at 65 y:<br />
cont<strong>in</strong>ue till 75 y. For 3:<br />
lifetime FU colonoscopy<br />
warranted (level 4).<br />
6. A completely resected<br />
adenoma does not recur<br />
(level 4).<br />
7. All resected polyps need<br />
histological exam<strong>in</strong>ation<br />
before sett<strong>in</strong>g up a<br />
surveillance strategy (level<br />
4).<br />
8. DCBE for FU after<br />
polypectomy is <strong>in</strong>dicated if<br />
endoscopist doubts<br />
complete removal of all<br />
polyps (level 4).<br />
9. Patients <strong>with</strong> high risk<br />
family history of CRC:<br />
more frequent FU<br />
warranted (level 4).<br />
Inflammatory bowel disease<br />
(IBD)<br />
Miscellaneous<br />
Not <strong>in</strong>cluded Not <strong>in</strong>cluded














