Report in English with a Dutch summary (KCE reports 45A)
Report in English with a Dutch summary (KCE reports 45A) Report in English with a Dutch summary (KCE reports 45A)
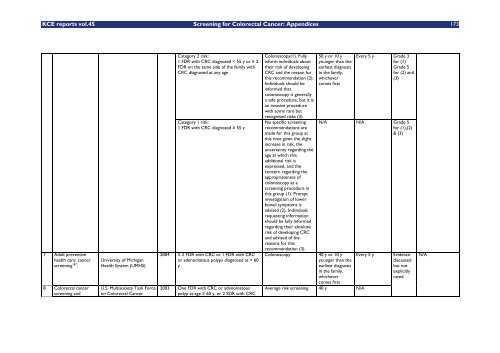
172 Screening for Colorectal Cancer: Appendices KCE reports vol.45 4 Guidelines for the Prevention, Early Detection and Management of Colorectal Cancer 50 5 American Cancer Society guidelines on screening and surveillance for the early detection of adenomatous polyps and colorectal cancer - update 200456 . 6 Surveillance and management of groups at increased risk of colorectal cancer27 . Australian Cancer Network Colorectal Cancer Guidelines Revision Committee American Cancer Society (ACS) New Zealand Guidelines Group (NZGG) 2005 1 FDR with CRC diagnosed at 55 years or over (included in category 1 RR up to 2-fold) 1 FDR with CRC diagnosed under 55 years (RR 3 to 6-fold) 2 FDR with CRC diagnosed at any age (RR 3 to 6-fold) 2004 Either CRC or adenomatous polyps in any FDR < 60 y, or in 2 FDR at any age (if not a hereditary syndrome). CRC in relatives more distant than FDR does not increase risk substantially above the average risk group 2004 Category 3 risk: 1 FDR plus 2 FDR or SDR, all on the same side of the family, with a diagnosis or CRC at any age 2 FDR, or 1 FDR plus 1 SDR, all on the same side of the family, with a diagnosis of CRC and one such relative (1) was diagnosed with CRC under age of 55 y, (2) developed multiple bowel cancers, or (3) developed an extra-colonic tumor suggestive of hereditary nonpolyposis colorectal cancer (i.e., endometrial, ovarian, stomach, small bowel, upper renal tract, pancreas, or brain) At least 1 FDR or SDR diagnosed with CRC in association with multiple bowel polyps 1 FDR with CRC diagnosed < 50 y, particularly if colorectal tumor immunohistochemistry has revealed loss of protein expression for one of the mismatch repair genes (hMLH1 or hMSH2) Colonoscopy FS and DCBE or CT colonography may be offered if colonoscopy is contraindicated for some reason. 50 y. or 10 years younger than the age of first diagnosis of bowel cancer in the family, whichever comes first. Colonoscopy Age 40, or 10 y before the youngest case in the immediate family Suspect hereditary disease and refer patient to: A genetic specialist/family cancer clinic or familial bowel cancer registry for further risk assessment and possible genetic testing If yes see surveillance; if no colonoscopy 40 y or 10 y younger than affected relative (whichever is younger), Repeat every 5 y. Every 5-10 y Evidence discussed but not explicitly rated Repeat every 1-5 y III-2 Recommended Grade 5 N/A See Appendix 2 NZGG National Health Committee evidence grading hierarchy
KCE reports vol.45 Screening for Colorectal Cancer: Appendices 173 7 Adult preventive health care: cancer screening 187 . 8 Colorectal cancer screening and University of Michigan Health System (UMHS) U.S. Multisociety Task Force on Colorectal Cancer Category 2 risk: 1 FDR with CRC diagnosed < 55 y or 2 FDR on the same side of the family with CRC diagnosed at any age Category 1 risk: 1 FDR with CRC diagnosed 55 y 2004 2 FDR with CRC or 1 FDR with CRC or adenomatous polyps diagnosed at < 60 y 2003 One FDR with CRC or adenomatous polyp at age 60 y, or 2 SDR with CRC Colonoscopy(1). Fully inform individuals about their risk of developing CRC and the reason for this recommendation (2). Individuals should be informed that colonoscopy is generally a safe procedure, but it is an invasive procedure with some rare but recognised risks (3). No specific screening recommendations are made for this group at this time given the slight increase in risk, the uncertainty regarding the age at which this additional risk is expressed, and the concern regarding the appropriateness of colonoscopy as a screening procedure in this group (1). Prompt investigation of lower bowel symptoms is advised (2). Individuals requesting information should be fully informed regarding their absolute risk of developing CRC and advised of the reasons for this recommendation (3). 50 y or 10 y younger than the earliest diagnosis in the family, whichever comes first Every 5 y Grade 3 for (1) Grade 5 for (2) and (3) N/A N/A Grade 5 for (1),(2) & (3) Colonoscopy 40 y or 10 y younger than the earliest diagnosis in the family, whichever comes first Every 5 y Average risk screening 40 y N/A Evidence discussed but not explicitly rated N/A
- Page 132 and 133: 122 Screening for Colorectal Cancer
- Page 134 and 135: 124 Screening for Colorectal Cancer
- Page 136 and 137: 126 Screening for Colorectal Cancer
- Page 138 and 139: 128 Screening for Colorectal Cancer
- Page 140 and 141: 130 Screening for Colorectal Cancer
- Page 142 and 143: 132 Screening for Colorectal Cancer
- Page 144 and 145: 134 Screening for Colorectal Cancer
- Page 146 and 147: 136 Screening for Colorectal Cancer
- Page 148 and 149: 138 Screening for Colorectal Cancer
- Page 150 and 151: 140 Screening for Colorectal Cancer
- Page 152 and 153: 142 Screening for Colorectal Cancer
- Page 154 and 155: 144 Screening for Colorectal Cancer
- Page 156 and 157: 146 Screening for Colorectal Cancer
- Page 158 and 159: 148 Screening for Colorectal Cancer
- Page 160 and 161: 150 Screening for Colorectal Cancer
- Page 162 and 163: 152 Screening for Colorectal Cancer
- Page 164 and 165: 154 Screening for Colorectal Cancer
- Page 166 and 167: 156 Screening for Colorectal Cancer
- Page 168 and 169: 158 Screening for Colorectal Cancer
- Page 170 and 171: 160 Screening for Colorectal Cancer
- Page 172 and 173: 162 Screening for Colorectal Cancer
- Page 174 and 175: 164 Screening for Colorectal Cancer
- Page 176 and 177: 166 Screening for Colorectal Cancer
- Page 178 and 179: 168 Screening for Colorectal Cancer
- Page 180 and 181: 170 Screening for Colorectal Cancer
- Page 184 and 185: 174 Screening for Colorectal Cancer
- Page 186 and 187: 176 Screening for Colorectal Cancer
- Page 188 and 189: 178 Screening for Colorectal Cancer
- Page 190 and 191: 180 Screening for Colorectal Cancer
- Page 192 and 193: 182 Screening for Colorectal Cancer
- Page 194 and 195: 184 Screening for Colorectal Cancer
- Page 196 and 197: 186 Screening for Colorectal Cancer
- Page 198 and 199: 188 Screening for Colorectal Cancer
- Page 200 and 201: 190 Screening for Colorectal Cancer
- Page 202 and 203: 192 Screening for Colorectal Cancer
- Page 204 and 205: 194 Screening for Colorectal Cancer
- Page 206 and 207: 196 Screening for Colorectal Cancer
- Page 208 and 209: 198 Screening for Colorectal Cancer
- Page 210 and 211: 200 Screening for Colorectal Cancer
- Page 212 and 213: 202 Screening for Colorectal Cancer
- Page 214 and 215: 204 Screening for Colorectal Cancer
- Page 216 and 217: 206 Screening for Colorectal Cancer
- Page 218 and 219: 208 Screening for Colorectal Cancer
- Page 220 and 221: 210 Screening for Colorectal Cancer
- Page 222 and 223: 212 Screening for Colorectal Cancer
- Page 224 and 225: 214 Screening for Colorectal Cancer
- Page 226 and 227: 216 Screening for Colorectal Cancer
- Page 228 and 229: 218 Screening for Colorectal Cancer
- Page 230 and 231: 220 Screening for Colorectal Cancer
<strong>KCE</strong> <strong>reports</strong> vol.45 Screen<strong>in</strong>g for Colorectal Cancer: Appendices 173<br />
7 Adult preventive<br />
health care: cancer<br />
screen<strong>in</strong>g 187 .<br />
8 Colorectal cancer<br />
screen<strong>in</strong>g and<br />
University of Michigan<br />
Health System (UMHS)<br />
U.S. Multisociety Task Force<br />
on Colorectal Cancer<br />
Category 2 risk:<br />
1 FDR <strong>with</strong> CRC diagnosed < 55 y or 2<br />
FDR on the same side of the family <strong>with</strong><br />
CRC diagnosed at any age<br />
Category 1 risk:<br />
1 FDR <strong>with</strong> CRC diagnosed 55 y<br />
2004 2 FDR <strong>with</strong> CRC or 1 FDR <strong>with</strong> CRC<br />
or adenomatous polyps diagnosed at < 60<br />
y<br />
2003 One FDR <strong>with</strong> CRC or adenomatous<br />
polyp at age 60 y, or 2 SDR <strong>with</strong> CRC<br />
Colonoscopy(1). Fully<br />
<strong>in</strong>form <strong>in</strong>dividuals about<br />
their risk of develop<strong>in</strong>g<br />
CRC and the reason for<br />
this recommendation (2).<br />
Individuals should be<br />
<strong>in</strong>formed that<br />
colonoscopy is generally<br />
a safe procedure, but it is<br />
an <strong>in</strong>vasive procedure<br />
<strong>with</strong> some rare but<br />
recognised risks (3).<br />
No specific screen<strong>in</strong>g<br />
recommendations are<br />
made for this group at<br />
this time given the slight<br />
<strong>in</strong>crease <strong>in</strong> risk, the<br />
uncerta<strong>in</strong>ty regard<strong>in</strong>g the<br />
age at which this<br />
additional risk is<br />
expressed, and the<br />
concern regard<strong>in</strong>g the<br />
appropriateness of<br />
colonoscopy as a<br />
screen<strong>in</strong>g procedure <strong>in</strong><br />
this group (1). Prompt<br />
<strong>in</strong>vestigation of lower<br />
bowel symptoms is<br />
advised (2). Individuals<br />
request<strong>in</strong>g <strong>in</strong>formation<br />
should be fully <strong>in</strong>formed<br />
regard<strong>in</strong>g their absolute<br />
risk of develop<strong>in</strong>g CRC<br />
and advised of the<br />
reasons for this<br />
recommendation (3).<br />
50 y or 10 y<br />
younger than the<br />
earliest diagnosis<br />
<strong>in</strong> the family,<br />
whichever<br />
comes first<br />
Every 5 y Grade 3<br />
for (1)<br />
Grade 5<br />
for (2) and<br />
(3)<br />
N/A N/A Grade 5<br />
for (1),(2)<br />
& (3)<br />
Colonoscopy 40 y or 10 y<br />
younger than the<br />
earliest diagnosis<br />
<strong>in</strong> the family,<br />
whichever<br />
comes first<br />
Every 5 y<br />
Average risk screen<strong>in</strong>g 40 y N/A<br />
Evidence<br />
discussed<br />
but not<br />
explicitly<br />
rated<br />
N/A


