

Non-specific neck pain: diagnosis and treatment - KCE
Non-specific neck pain: diagnosis and treatment - KCE
Non-specific neck pain: diagnosis and treatment - KCE

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
30 <strong>Non</strong>-Specific Neck Pain: <strong>diagnosis</strong> <strong>and</strong> <strong>treatment</strong> <strong>KCE</strong> Reports 119<br />
5 SUMMARY<br />
History taking<br />
Excluding red flags<br />
Diagnostic imaging<br />
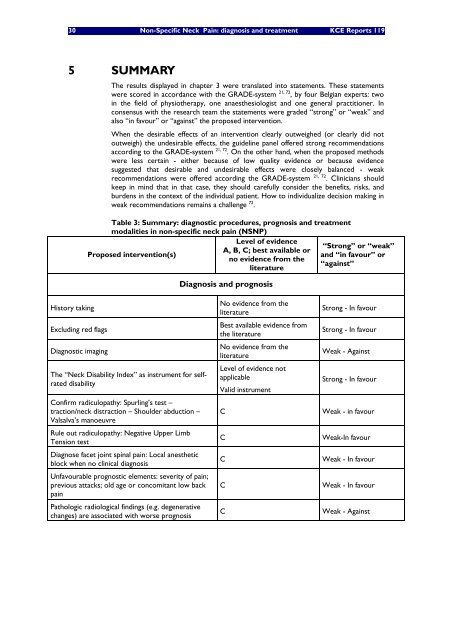
The results displayed in chapter 3 were translated into statements. These statements<br />
were scored in accordance with the GRADE-system 21, 72 , by four Belgian experts: two<br />
in the field of physiotherapy, one anaesthesiologist <strong>and</strong> one general practitioner. In<br />
consensus with the research team the statements were graded “strong” or “weak” <strong>and</strong><br />
also “in favour” or “against” the proposed intervention.<br />
When the desirable effects of an intervention clearly outweighed (or clearly did not<br />
outweigh) the undesirable effects, the guideline panel offered strong recommendations<br />
according to the GRADE-system 21, 72 . On the other h<strong>and</strong>, when the proposed methods<br />
were less certain - either because of low quality evidence or because evidence<br />
suggested that desirable <strong>and</strong> undesirable effects were closely balanced - weak<br />
recommendations were offered according the GRADE-system 21, 72 . Clinicians should<br />
keep in mind that in that case, they should carefully consider the benefits, risks, <strong>and</strong><br />
burdens in the context of the individual patient. How to individualize decision making in<br />
weak recommendations remains a challenge 72 .<br />
Table 3: Summary: diagnostic procedures, prognosis <strong>and</strong> <strong>treatment</strong><br />
modalities in non-<strong>specific</strong> <strong>neck</strong> <strong>pain</strong> (NSNP)<br />
Level of evidence<br />
“Strong” or “weak”<br />
A, B, C; best available or<br />
Proposed intervention(s)<br />
<strong>and</strong> “in favour” or<br />
no evidence from the<br />
“against”<br />
literature<br />
The “Neck Disability Index” as instrument for selfrated<br />
disability<br />
Confirm radiculopathy: Spurling’s test –<br />
traction/<strong>neck</strong> distraction – Shoulder abduction –<br />
Valsalva’s manoeuvre<br />
Rule out radiculopathy: Negative Upper Limb<br />
Tension test<br />
Diagnose facet joint spinal <strong>pain</strong>: Local anesthetic<br />
block when no clinical <strong>diagnosis</strong><br />
Unfavourable prognostic elements: severity of <strong>pain</strong>;<br />
previous attacks; old age or concomitant low back<br />
<strong>pain</strong><br />
Pathologic radiological findings (e.g. degenerative<br />
changes) are associated with worse prognosis<br />
Diagnosis <strong>and</strong> prognosis<br />
No evidence from the<br />
literature<br />
Best available evidence from<br />
the literature<br />
No evidence from the<br />
literature<br />
Level of evidence not<br />
applicable<br />
Valid instrument<br />
Strong - In favour<br />
Strong - In favour<br />
Weak - Against<br />
Strong - In favour<br />
C Weak - in favour<br />
C Weak-In favour<br />
C Weak - In favour<br />
C Weak - In favour<br />
C Weak - Against














