ehr onc final certification - Department of Health Care Services
ehr onc final certification - Department of Health Care Services ehr onc final certification - Department of Health Care Services
include a capability and how it must perform the capability. As a result, it is not within the scope of this rulemaking to specify the persons who would need to use CPOE. Comment. A commenter suggested that we not create controlled vocabularies or value sets in the regulation but rather refer to and adopt existing controlled vocabularies or subsets. The commenter also stated that the regulation introduces a requirement to record, store, retrieve and manage orders, though no vocabularies are specified and further pointed out that there are no vocabularies or standards for orders, images, or referrals in any part of the Interim Final Rule. The commenter recommended that the Department focus its efforts on identifying and adopting standards for computable and interoperable representations of these elements and processes before directing eligible professionals to implement “CPOE.” Response. We appreciate the commenter’s concern. This is an initial set of standards, implementation specifications, and certification criteria and we expect to adopt more standards, implementation specifications, and certification criteria in the future as necessary to improve the comprehensiveness of certain capabilities. Comment. A commenter requested that we clarify whether only imaging and radiology reports were intended to be included in this capability, or, if we intended to include the images themselves in addition to the imaging reports as part of the certification criteria. The commenter recommended that we further clarify the criterion and moreover, adopt the DICOM standard in the initial set of standards, as an essential step in meeting the CPOE capability. Response. We clarify that the adopted certification criteria related to CPOE pertain only to the ordering, and not to the delivery of results (reports or images). As a Page 128 of 228
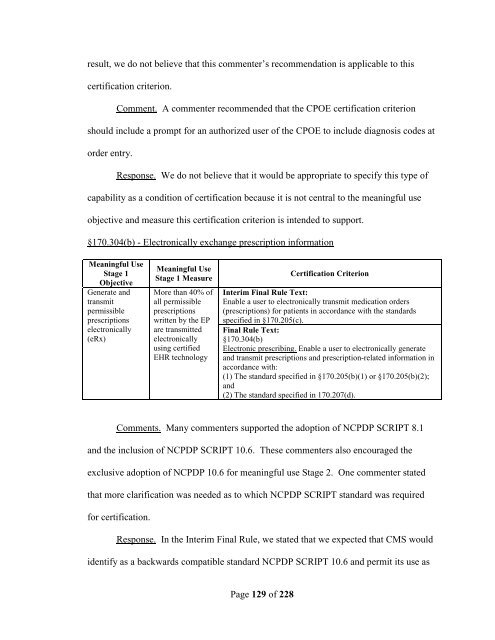
esult, we do not believe that this commenter’s recommendation is applicable to this certification criterion. Comment. A commenter recommended that the CPOE certification criterion should include a prompt for an authorized user of the CPOE to include diagnosis codes at order entry. Response. We do not believe that it would be appropriate to specify this type of capability as a condition of certification because it is not central to the meaningful use objective and measure this certification criterion is intended to support. §170.304(b) - Electronically exchange prescription information Meaningful Use Stage 1 Objective Generate and transmit permissible prescriptions electronically (eRx) Meaningful Use Stage 1 Measure More than 40% of all permissible prescriptions written by the EP are transmitted electronically using certified EHR technology Page 129 of 228 Certification Criterion Interim Final Rule Text: Enable a user to electronically transmit medication orders (prescriptions) for patients in accordance with the standards specified in §170.205(c). Final Rule Text: §170.304(b) Electronic prescribing. Enable a user to electronically generate and transmit prescriptions and prescription-related information in accordance with: (1) The standard specified in §170.205(b)(1) or §170.205(b)(2); and (2) The standard specified in 170.207(d). Comments. Many commenters supported the adoption of NCPDP SCRIPT 8.1 and the inclusion of NCPDP SCRIPT 10.6. These commenters also encouraged the exclusive adoption of NCPDP 10.6 for meaningful use Stage 2. One commenter stated that more clarification was needed as to which NCPDP SCRIPT standard was required for certification. Response. In the Interim Final Rule, we stated that we expected that CMS would identify as a backwards compatible standard NCPDP SCRIPT 10.6 and permit its use as
- Page 77 and 78: months). We believe that these revi
- Page 79 and 80: that the PQRI 2009 Registry XML spe
- Page 81 and 82: To better align this certification
- Page 83 and 84: the capability specified by the cer
- Page 85 and 86: vendors were unwilling or unable to
- Page 87 and 88: the concerns expressed by some comm
- Page 89 and 90: Page 89 of 228 electronically compa
- Page 91 and 92: (1) The standard (and applicable im
- Page 93 and 94: for the purposes of demonstrating c
- Page 95 and 96: Guide for Immunization Messaging Re
- Page 97 and 98: Response. We clarify for commenters
- Page 99 and 100: serve as a limiting factor, however
- Page 101 and 102: Page 101 of 228 Unchanged Comment.
- Page 103 and 104: Comment. One commenter suggested th
- Page 105 and 106: Response. We appreciate the thought
- Page 107 and 108: Complete EHRs or EHR Modules design
- Page 109 and 110: Response. We disagree. As stated ab
- Page 111 and 112: Response. As discussed above, we ha
- Page 113 and 114: SHA-1 and other secure hash algorit
- Page 115 and 116: misinterpreted our example and stat
- Page 117 and 118: Other commenters also expressed con
- Page 119 and 120: eferenced in FIPS 140-2 Annex A, wh
- Page 121 and 122: of the most secure encryption algor
- Page 123 and 124: the disclosure was made (recipient)
- Page 125 and 126: Use CPOE for medication orders dire
- Page 127: equire EHRs to build custom interfa
- Page 131 and 132: was needed before RxNorm could be a
- Page 133 and 134: • MDDB - Medi-Span Master Drug Da
- Page 135 and 136: Response. We do not believe that it
- Page 137 and 138: Send reminders to patients per pati
- Page 139 and 140: specified data elements and CMS’s
- Page 141 and 142: what would qualify as a "response."
- Page 143 and 144: Comment. A commenter recommended th
- Page 145 and 146: in accordance with one of the adopt
- Page 147 and 148: Comments. Many commenters suggested
- Page 149 and 150: flexibility in this certification c
- Page 151 and 152: productive, confusing, time-consumi
- Page 153 and 154: include in this initial set. Accord
- Page 155 and 156: to the HITSP C32 implementation spe
- Page 157 and 158: Response. Again, we do not believe
- Page 159 and 160: e achieved without these and recomm
- Page 161 and 162: electronically record, store, retri
- Page 163 and 164: EHRs and EHR Modules designed for a
- Page 165 and 166: §170.205(a)(2)(iii); and (v) The s
- Page 167 and 168: Response. We disagree, as doing so
- Page 169 and 170: Dental Terminology as a condition o
- Page 171 and 172: However, we do not preclude Complet
- Page 173 and 174: ability of CCD and CCR to support t
- Page 175 and 176: ability to receive these reports. M
- Page 177 and 178: commenters acknowledged and express
esult, we do not believe that this commenter’s recommendation is applicable to this<br />
<strong>certification</strong> criterion.<br />
Comment. A commenter recommended that the CPOE <strong>certification</strong> criterion<br />
should include a prompt for an authorized user <strong>of</strong> the CPOE to include diagnosis codes at<br />
order entry.<br />
Response. We do not believe that it would be appropriate to specify this type <strong>of</strong><br />
capability as a condition <strong>of</strong> <strong>certification</strong> because it is not central to the meaningful use<br />
objective and measure this <strong>certification</strong> criterion is intended to support.<br />
§170.304(b) - Electronically exchange prescription information<br />
Meaningful Use<br />
Stage 1<br />
Objective<br />
Generate and<br />
transmit<br />
permissible<br />
prescriptions<br />
electronically<br />
(eRx)<br />
Meaningful Use<br />
Stage 1 Measure<br />
More than 40% <strong>of</strong><br />
all permissible<br />
prescriptions<br />
written by the EP<br />
are transmitted<br />
electronically<br />
using certified<br />
EHR technology<br />
Page 129 <strong>of</strong> 228<br />
Certification Criterion<br />
Interim Final Rule Text:<br />
Enable a user to electronically transmit medication orders<br />
(prescriptions) for patients in accordance with the standards<br />
specified in §170.205(c).<br />
Final Rule Text:<br />
§170.304(b)<br />
Electronic prescribing. Enable a user to electronically generate<br />
and transmit prescriptions and prescription-related information in<br />
accordance with:<br />
(1) The standard specified in §170.205(b)(1) or §170.205(b)(2);<br />
and<br />
(2) The standard specified in 170.207(d).<br />
Comments. Many commenters supported the adoption <strong>of</strong> NCPDP SCRIPT 8.1<br />
and the inclusion <strong>of</strong> NCPDP SCRIPT 10.6. These commenters also encouraged the<br />
exclusive adoption <strong>of</strong> NCPDP 10.6 for meaningful use Stage 2. One commenter stated<br />
that more clarification was needed as to which NCPDP SCRIPT standard was required<br />
for <strong>certification</strong>.<br />
Response. In the Interim Final Rule, we stated that we expected that CMS would<br />
identify as a backwards compatible standard NCPDP SCRIPT 10.6 and permit its use as


