Changing MIC Breakpoints: Do Mechanisms Count
Changing MIC Breakpoints: Do Mechanisms Count
Changing MIC Breakpoints: Do Mechanisms Count

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Changing</strong> <strong>MIC</strong> <strong>Breakpoints</strong>:<br />
<strong>Do</strong> <strong>Mechanisms</strong> <strong>Count</strong><br />
Paul C. Schreckenberger, Ph.D., D(ABMM), F(AAM)<br />
Professor of Pathology<br />
Director, Clinical Microbiology Laboratory<br />
Loyola University Medical Center<br />
pschrecken@lumc.edu
YES
• The major issue is whether the new<br />
Enterobacteriaceae <strong>MIC</strong> breakpoints can<br />
predict clinical success and failure even<br />
without ancillary tests or whether laboratories<br />
need to continue to screen for, and confirm<br />
the presence or absence of ESBLs and<br />
Carbapenemases before issuing a<br />
susceptibility report<br />
3
CLSI Guidelines<br />
• CLSI has history of recommending testing for<br />
mechanisms in order to detect false susceptible<br />
results with in vitro testing<br />
Staph spp. Table 2C p. 69 M100-S21<br />
• Detection of oxacillin Resistance: Tests for mecA<br />
or PBP2a are the most accurate methods for<br />
prediction of resistance to oxacillin ….. Isolates<br />
that carry the mecA or PBP2a should be reported<br />
“oxacillin resistant”<br />
Staph spp. Table 2C p. 76,79 M100-S21<br />
• Inducible clindamycin rsistance can be detected by<br />
disk diffusion using the D-zone test ….. Report<br />
isolates with inducible clindamycin resistance as<br />
“clindamycin resistant”<br />
4
CLSI Guidelines<br />
Staph spp. Table 2C p. 70,78 M100-S21<br />
• An induced -lactamase test should be performed<br />
on staphylococcal isolates with penicillin <strong>MIC</strong>s<br />
0.12 ug/ml or zone dia. 29 mm before reporting<br />
isolate as penicillin susceptible …. A positive -<br />
lactamase test predicts resistance to penicillin.<br />
5
CLSI Guidance on ESBL Testing<br />
• Will Tests for ESBLs and KPCs be needed with<br />
the new cephalosporin and carbapenem<br />
breakpoints for Enterobacteriaceae?<br />
CLSI says No. For patient management,<br />
tests for ESBLs and KPCs are not necessary<br />
If requested, tests for ESBLs and KPCs may<br />
be done for Infection Control purposes<br />
6
New CLSI Guidelines 2010<br />
• This decision was based on evaluation of<br />
pharmacokinetics-pharmacodynamics (PK-PD)<br />
properties and limited clinical trials<br />
• New interpretive criteria (breakpoints) establish<br />
for some (but not all) cephalosporins<br />
• Using new breakpoints treatment decisions can<br />
be based solely on <strong>MIC</strong> alone<br />
• “It’s all about the <strong>MIC</strong> stupid”<br />
7
New CLSI Guidelines 2010<br />
• Problem with this approach<br />
Clinical studies show patients with<br />
“susceptible” <strong>MIC</strong>s + ESBL fail therapy<br />
8
Clinical Studies<br />
• No randomized controlled trials have ever<br />
been performed that evaluated the use of<br />
various comparator antibiotics in treatment of<br />
serious infections due to ESBL-producing<br />
organisms<br />
• It is unlikely that such studies will ever be<br />
performed<br />
• Existing data comes only from retrospective<br />
studies<br />
9
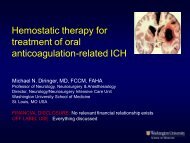
Treatment of ESBL Positive<br />
Organisms with Cephalosporins<br />
<strong>MIC</strong> FAILURE DEATH<br />
8 100% (6/6) 33% (2/6)<br />
4 67% (2/3) 0% (0/3)<br />
2 33% (1/3) 0% (0/3)<br />
≤1 27% (3/11) 18% (2/11)<br />
(CLSI breakpoint 8 g/ml)<br />
Paterson, DL, et al. JCM 39: 2206 – 2212, 2001<br />
10
New CLSI Guidelines 2010<br />
• Problem with this approach<br />
Clinical studies show patients with “susceptible”<br />
<strong>MIC</strong>s + ESBL fail therapy<br />
Inoculum used in bmd (10 5 ) too low and may<br />
dilute out resistant subpopulations giving<br />
false susceptible results<br />
11
<strong>MIC</strong>s in g/ml: SHV-3 producing Citrobacter freundii<br />
Inocul.<br />
CFU/ml<br />
Pitfalls of ESBL Testing<br />
Effects of Inoculum<br />
Cefotaxime Ceftazidime Aztreonam Cefepime<br />
5 x 10 5 2 1 0.5 0.5<br />
(CLSI breakpoint 8 g/ml)<br />
Thomson KS, Moland ES: Antimicrob Agents<br />
Chemother. 2001 Dec;45(12):3548-54<br />
12
<strong>MIC</strong>s in g/ml: SHV-3 producing Citrobacter freundii<br />
Inocul.<br />
CFU/ml<br />
Pitfalls of ESBL Testing<br />
Effects of Inoculum<br />
Cefotaxime Ceftazidime Aztreonam Cefepime<br />
5 x 10 5 2 1 0.5 0.5<br />
5 x 10 7 256 32 32 >1024<br />
(CLSI breakpoint 8 g/ml)<br />
Thomson KS, Moland ES: Antimicrob Agents<br />
Chemother. 2001 Dec;45(12):3548-54<br />
13
Inoculum Effect<br />
• Animal studies also demonstrate an inoculum<br />
effect and adverse outcomes when<br />
cephalosporins are used to treat ESBLproducing<br />
organisms with <strong>MIC</strong>s of<br />
cephalosporin in the susceptible range.<br />
14
Efficacy of different beta-lactams against an<br />
ESBL-producing K. pneumoniae in rat IAA Model<br />
• Abscess created by intraperitoneal placement gelatin<br />
capsule containing sterile rat cecal contents, killed B.<br />
fragilis, and 1:100 dilution of ESBL-K. pneumonia (ca.<br />
10 5 CFU)<br />
• Treatment begun by continuous infusion via left internal<br />
jugular vein 3-4 hours after placement of capsule and<br />
continued 3 days.<br />
• On day 2 and 3 blood samples were collected for<br />
determination of serum antibiotic levels<br />
• After 3 days animals were sacrificed, abdominal wall<br />
portion of abscess removed and quantitative culture<br />
performed<br />
Rice LB et al. Antimicrob Agents Chemother.<br />
1991 Jun;35(6):1243-4.<br />
15
Efficacy of different beta-lactams against an<br />
ESBL-producing K. pneumoniae in rat IAA Model<br />
Table 1: <strong>MIC</strong>s of various agents for K. pneumoniae 5657<br />
Antimicrobial Agent <strong>MIC</strong> at inoculum of:<br />
10 5 CFU/ml 10 7 CFU/ml<br />
Cefoperazone 2 256<br />
Sulbactam 32<br />
Cefoperazone-sulbactam (2:1) 0.5 256<br />
Cefotaxime 1 256<br />
Cefpirome 1 >256<br />
Ceftazidime >256<br />
Imipenem 0.5 16<br />
Rice LB et al. Antimicrob Agents Chemother.<br />
1991 Jun;35(6):1243-4.<br />
16
Efficacy of different beta-lactams against an<br />
ESBL-producing K. pneumoniae in rat IAA model<br />
Table 2: Intra-abdominal abscess treatment outcomes<br />
Antibiotic No.<br />
rats<br />
Mean serum<br />
level ( g/ml)<br />
Log10<br />
CFU/g of<br />
abscess<br />
None 30 8.02 1.02<br />
Cefoperazone 11 13.5 4.72 7.41 0.74 a<br />
Cefoperazone-sulbactam 11 8.9 3.22 5.84 0.95 c<br />
Cefotaxime 18 17.7 8.42 7.26 1.02 a<br />
Cefpirome 11 28.3 2.06 7.80 1.18 a<br />
Ceftazidime 10 19.4 3.09 8.85 0.64 a<br />
Imipenem 19 7.1 2.08 4.99 0.97 c<br />
a P>0.05, c P
Efficacy of different beta-lactams against an<br />
ESBL-producing K. pneumoniae in rat IAA model<br />
• Conclusions<br />
Extend spectrum cephalosporins may be less<br />
effective in treating serious infections due to<br />
ESBL producing gram-negative bacilli than<br />
standard susceptibility tests would imply<br />
In vitro studies indicated that the activity of<br />
these agents against K. pneumoniae 5657<br />
was highly inoculum dependent<br />
Rice LB et al. Antimicrob Agents Chemother.<br />
1991 Jun;35(6):1243-4.<br />
18
Efficacy of different beta-lactams against an<br />
ESBL-producing K. pneumoniae in rat IAA model<br />
• Conclusions<br />
Dramatic improvement of in vivo efficacy of<br />
cefoperazone in presence of sulbactam was<br />
due at least in part to presence of<br />
-lactamase<br />
Avoid extended spectrum cephalosporins<br />
as single agents when treating serious<br />
infections with ESBL-producing<br />
organisms<br />
Rice LB et al. Antimicrob Agents Chemother.<br />
1991 Jun;35(6):1243-4.<br />
19
New CLSI Guidelines 2010<br />
• Problem with this approach<br />
Clinical studies show patients with “susceptible”<br />
<strong>MIC</strong>s + ESBL fail therapy<br />
Inoculum used in bmd (10 5 ) too low and may dilute<br />
out resistant subpopulations giving false susceptible<br />
results<br />
Different susceptibility testing methods give<br />
varying results<br />
20
CAP Survey D-C 2007 D-19<br />
C. freundii with PER-1 ESBL with <strong>MIC</strong> 16 g/ml<br />
Method/system<br />
tested (no.)<br />
Reported Cefepime<br />
<strong>MIC</strong> or zone in<br />
Susceptible category<br />
BD Phoenix (24) Not reported >16<br />
MicroScan (311) 15% >16<br />
Vitek (244) 97.2% 4<br />
Vitek 2 (230) 85.5% 2<br />
Final Critique Survey 2007 D-C<br />
College of American Pathologists<br />
Modal <strong>MIC</strong><br />
Disk Diffusion (74) 34% 15.5 mm<br />
21
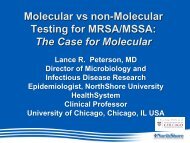
CAP Survey D-A 2009 D-05<br />
K. pneumoniae KPC with <strong>MIC</strong> ≥8 g/ml<br />
Carbabenem/<br />
system tested<br />
(no.)<br />
No. Reports By Category<br />
Imipenem S I R Modal<br />
<strong>MIC</strong> g/ml<br />
BD Phoenix (24) 4 (17%) 7 13 >8<br />
MicroScan (538) 73 (14%) 217 248 8<br />
Vitek (154) 111 (72%) 10 33 ≤4<br />
Vitek 2 (422) 44 (10%) 6 372 2<br />
Final Critique Survey 2009 D-A<br />
College of American Pathologists<br />
22
New CLSI Guidelines 2010<br />
• Problem with this approach<br />
Clinical studies show patients with “susceptible” <strong>MIC</strong>s + ESBL<br />
fail therapy<br />
Inoculum used in bmd (10 5 ) too low and may dilute out resistant<br />
subpopulations giving false susceptible results<br />
Different susceptibility testing methods give varying results<br />
<strong>MIC</strong> results are not reproducible and can very up to<br />
>3 dilutions upon repeat testing<br />
23
CLSI Acceptable Limits ( g/mL) for QC<br />
Strains Used to Monitor Accuracy<br />
Antimicrobial E. Coli ATCC 25922 No. of <strong>Do</strong>ubling<br />
Dilutions Allowed<br />
Cefazolin 1-4 3<br />
Cefotaxime 0.03-0.12 3<br />
Ceftriaxone 0.03-0.12 3<br />
Ceftazidime 0.06-0.5 4<br />
Aztreonam 0.06-0.25 3<br />
Cefepime 0.015-0.12 8<br />
CLSI M100-S20. Table 4<br />
24
<strong>MIC</strong> Reproducibility<br />
• In this imperfect reality an ESBL producer<br />
with a cefotaxime <strong>MIC</strong> of 1 g/mL (probably<br />
responsive to cefotaxime in vivo) cannot be<br />
reliably distinguished from one with an <strong>MIC</strong> of<br />
4 g/mL (probably not responsive) and it is<br />
simpler and safer to follow the precautionary<br />
approach of seeking the ESBL and, if found,<br />
reporting the isolate as resistant<br />
- David Livermore, 20 th European Congress of<br />
Clinical Microbiology and Infectious Diseases,<br />
Vienna, Austria, 10-13 April, 2010.<br />
25
New CLSI Guidelines 2010<br />
• Problem with this approach<br />
Clinical studies show patients with “susceptible” <strong>MIC</strong>s + ESBL<br />
fail therapy<br />
Inoculum used in bmd (10 5 ) too low and may dilute out resistant<br />
subpopulations giving false susceptible results<br />
Different susceptibility testing methods give varying results<br />
<strong>MIC</strong> results are not reproducible and can very up to 3 dilutions<br />
upon repeat testing<br />
Some cephalosporin breakpoints were not lowered<br />
enough and others not lowered at all<br />
26
Enterobacteriaceae<br />
Revised <strong>Breakpoints</strong> (<strong>MIC</strong> g.ml)<br />
Agent CLSI M100-S19<br />
(2009)<br />
CLSI M100-S20<br />
(2010)<br />
Susc Int Res Susc Int Res<br />
Cefazolin 8 16 32 1 2 4<br />
Cefotaxime 8 16-32 64 1 2 4<br />
Ceftizoxime 8 16-32 64 1 2 4<br />
Ceftriaxone 8 16-32 64 1 2 4<br />
Ceftazidime 8 16 32 4 8 16<br />
Aztreonam 8 16 32 4 8 16<br />
CLSI M100-S20. Table 2A<br />
27
Enterobacteriaceae – Evaluated<br />
but NOT Revised <strong>Breakpoints</strong><br />
Agent CLSI M100-S20 (2010)<br />
Cefuroxime<br />
(parenteral)<br />
Susc Int Res<br />
8 16 32<br />
Cefepime 8 16 32<br />
Cefotetan 16 32 64<br />
Cefoxitin 8 16 32<br />
CLSI M100-S20. Table 2A<br />
28
Cephaloporin <strong>Breakpoints</strong> Following<br />
Recent EUCAST and CLSI Revisions<br />
Group Cefuroxime<br />
S /R><br />
Cefotaxime<br />
S /R><br />
Ceftriaxone<br />
S /R><br />
Ceftazidime<br />
S /R><br />
Cefepime<br />
S /R><br />
CLSI 8/8 1/2 1/2 4/8 8/16<br />
EUCAST 8/8 1/2 1/2 1/8 a 1/8 a<br />
EUCAST<br />
PK/PD<br />
4/8 1/2 1/2 4/8 4/8<br />
a Ceftazidime and cefepime S breakpoints were adjusted from 4 to 1 ug/ml to<br />
ensure that Enterobacteriaceae with clinically important ESBLs were not<br />
reported as susceptible<br />
Kahlmeter G Clin Microbiol Infect. 2008 Jan;14 Suppl<br />
1:169-74. Review<br />
29
Enterobacteriaceae epidemiologic<br />
cut-off values (wild type X g/mL)<br />
E. coli K. pneumoniae K. oxytoca P. mirabilis<br />
Cefuroxime 8 8 8 4<br />
Cefotaxime 0.25 0.12 0.12 0.06<br />
Ceftriaxone 0.25 0.12 0.12 0.06<br />
Ceftaxidime 0.5 0.5 0.5 0.12<br />
Cefepime 0.12 0.12 0.12 0.12<br />
Kahlmeter G Clin Microbiol Infect. 2008 Jan;14 Suppl<br />
1:169-74. Review<br />
30
New CLSI Guidelines 2010<br />
• Problem with this approach<br />
Clinical studies show patients with “susceptible” <strong>MIC</strong>s + ESBL<br />
fail therapy<br />
Inoculum used in bmd (10 5 ) too low and may dilute out resistant<br />
subpopulations giving false susceptible results<br />
Different susceptibility testing methods give varying results<br />
<strong>MIC</strong> results are not reproducible and can very up to 3 dilutions<br />
upon repeat testing<br />
Some cephalosporin breakpoints were not lowered enough and<br />
others not lowered at all<br />
ESBL enzymes are substrate specific, may miss<br />
ESBL resistance if not testing the preferred substrate<br />
(eg. CTX-M)<br />
31
E. coli with CTX-M ESBL<br />
33
Why labs should continue to perform<br />
ESBL and KPC testing on all isolates<br />
•<strong>MIC</strong> results are inoculum dependent.<br />
•<strong>MIC</strong> results are not reproducible and can vary<br />
by >3 dilutions<br />
•Some ESBLs are inducible, ie. <strong>MIC</strong> is low initially<br />
but will test resistant after exposure to<br />
antibiotic. Presents a problem especially for<br />
Rapid Detection Methods<br />
•Knowing mechanism of resistance is important.<br />
It allows us to modify our reports and<br />
implement prompt infection control strategies<br />
34
Why labs should continue to perform<br />
ESBL and KPC testing on all isolates<br />
•Combining the lowering of <strong>MIC</strong><br />
breakpoints with ESBL and KPC confirmation<br />
testing gives the laboratory the best chance<br />
of getting the result right for the patient<br />
35
Are the New CLSI <strong>Breakpoints</strong><br />
the Correct <strong>Breakpoints</strong>?
Something to Think About<br />
• The <strong>MIC</strong> is only one piece of information that is<br />
useful in deciding if an antibiotic is going to be<br />
successful in treating an infection.<br />
• There will never be a single breakpoint that will<br />
predict susceptibility or resistance to a drug for<br />
all patients, at all sites of infection, and under all<br />
conditions based on the <strong>MIC</strong><br />
37
Something to Think About<br />
• <strong>Breakpoints</strong> can vary by infection type (e.g.,<br />
cystitis vs. sepsis vs. meningitis, etc.).<br />
• <strong>Breakpoints</strong> can vary by the method of antibiotic<br />
administration (e.g., oral vs. IV administration)<br />
or dosage given (customary vs. highest dose).<br />
• The FDA and CLSI breakpoints are based only<br />
on the drug level achieved in blood using the<br />
customary dose<br />
38
Something to Think About<br />
• In fact, the antibiotic reports issued by the<br />
laboratory are most often not for infections<br />
occurring in the blood (LUMC Feb ’11 87/813)<br />
• Drug concentrations at sites of infection<br />
outside blood stream may be higher or lower<br />
than those in blood, rendering the breakpoint<br />
less useful in these sites.<br />
39
Something to Think About<br />
• Antibiotics are often renally excreted and the<br />
renal function of the patient will determine<br />
how long the antibiotic will remain in the<br />
blood and how much is concentrated in other<br />
sites such as the bladder<br />
• In addition, all antibiotics are partially protein<br />
bound, so the albumin level of the patient<br />
affects the amount of free drug circulating.<br />
40
Time to Start Thinking Outside<br />
the Box – Eliminate <strong>Breakpoints</strong><br />
• I proposed a new approach for interpreting<br />
the results of AST, customized for each<br />
patient based on a number of factors<br />
41
Personalized Antibiotic Report<br />
• Customized for each patient based on:<br />
Organism ID<br />
<strong>MIC</strong><br />
Site of infection<br />
Drug concentration<br />
at site of infection<br />
Renal function<br />
Protein level<br />
Method of<br />
administration<br />
<strong>Do</strong>sing<br />
convenience<br />
Potential for D-D<br />
interactions<br />
Patient allergies<br />
Cost<br />
42
Personalized Antibiotic Report<br />
• To achieve this goal, sophisticated computer<br />
software would have to be developed that<br />
would customize reports for each patient by<br />
mining the EMR and using data on creatinine<br />
clearance, albumin concentration, site of<br />
infection, type of infection, culture results, and<br />
mode of antibiotic administration, to provide a<br />
personalized antibiotic report that would<br />
specify the optimal antibiotic(s) to treat the<br />
infection<br />
43
Personalized Antibiotic Report<br />
• Cost features, such as the need to perform<br />
therapeutic drug monitoring, drug-to-drug<br />
interactions, and in-patient or home therapy<br />
usage could also be incorporated into the<br />
computer algorithm<br />
We a teenager or a guy<br />
named Steve to step up<br />
and develop a computer<br />
application for this purpose<br />
44
Is it time to move past the<br />
concept of the universal<br />
breakpoint?<br />
Let’s Think About It
Are the New CLSI <strong>Breakpoints</strong><br />
the Correct <strong>Breakpoints</strong>?<br />
“There ain’t no answer. There<br />
ain’t going to be an answer.<br />
There never has been an<br />
answer. That’s the answer”<br />
- Gertrude Stein