Baha Candidate Selection Guide - Cochlear
Baha Candidate Selection Guide - Cochlear
Baha Candidate Selection Guide - Cochlear

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
A Bone ConduCtion HeAring Solution<br />
<strong>Candidate</strong><br />
<strong>Selection</strong> <strong>Guide</strong><br />
FOR PROFessiOnals
<strong>Candidate</strong> selection <strong>Guide</strong><br />
Products in this manual are protected by the following patents: US 5 735 790, US 5 7 935 170, EP 0715839, EP 0715838 and corresponding patents in other<br />
countries and pending patent applications. All products can be subject to change without notice. No part of this publication may be replaced, stored in a retrieval<br />
system, or transmitted in any form, by electronic, mechanical, photocopying, recording, or other means, without the prior written permission of the publisher.<br />
Caution: Federal law (USA) restricts this device to sale by or on the order of a medical practitioner.<br />
© <strong>Cochlear</strong> 2011. All rights reserved.<br />
Contents<br />
5 Introduction<br />
6 PART 1: Identifying candidates<br />
11 PART 2: <strong>Candidate</strong> evaluation<br />
14 PART 3: Counseling<br />
17 PART 4: Pediatric candidacy<br />
20 PART 5: Device considerations<br />
23 PART 6: Case histories<br />
28 PART 7: Clinical results<br />
29 References<br />
30 Notes<br />
<strong>Candidate</strong> selection <strong>Guide</strong><br />
2 3
introduction<br />
Introduction<br />
This <strong>Candidate</strong> <strong>Selection</strong> <strong>Guide</strong> provides detailed information<br />
on how to select candidates who will benefit from <strong>Cochlear</strong><br />
<strong>Baha</strong> ® 3 System. With bone conduction, sound bypasses the<br />
outer and middle ear, and goes directly to the nearest good<br />
inner ear. <strong>Baha</strong> is an effective implantable hearing solution for<br />
people with conductive hearing loss, mixed hearing loss, or<br />
single-sided sensorineural deafness (SSD). The <strong>Baha</strong> System<br />
works by enhancing natural bone conducted sound.<br />
the advantages of <strong>Baha</strong><br />
The main advantage of <strong>Baha</strong> is that it bypasses the conductive element of a hearing loss<br />
through direct bone conduction and only needs to compensate for the sensorineural element.<br />
Therefore, for conductive or mixed hearing loss with an air-bone gap >30 dB, measured at<br />
500, 1000, 2000, and 4000 Hz (PTA 4 ), <strong>Baha</strong> should be the amplification method of choice. 1-6<br />
For people with SSD the <strong>Baha</strong> is worn on the deaf side. When worn on the deaf side, the <strong>Baha</strong><br />
device transfers sound directly to the healthy cochlea, which reduces the effects of the head<br />
shadow effect, enables 360˚ sound awareness, and improves speech understanding in noise. 7-9<br />
There are also several medical indications where <strong>Baha</strong> could be the best solution for the<br />
candidate. Read more about this on page 10.<br />
Getting <strong>Baha</strong> for your candidate<br />
When you have identified a candidate for <strong>Baha</strong>, the candidate will need to be referred<br />
to an ENT surgeon for consultation. <strong>Candidate</strong>s considered suitable for surgery will then<br />
have a small titanium implant placed in the mastoid bone behind their ear.<br />
The <strong>Baha</strong> 3 System consists of a high-performance sound processor, an abutment and a<br />
titanium implant which is located in the bone behind the ear. The surgical procedure<br />
may be performed under a local anesthesia and is generally regarded as minor surgery from<br />
both the surgeon’s and candidate’s point of view. The <strong>Baha</strong> Sound Processor is easily<br />
connected and disconnected once the implant has fused with the bone (a process known<br />
as osseointegration).<br />
4 5<br />
introduction<br />
advantages of <strong>Baha</strong><br />
Compared to conventional air<br />
conduction (aC) hearing aids:<br />
• Less need for amplification<br />
because the conductive<br />
element of the hearing<br />
loss is bypassed<br />
• No occlusion of the<br />
ear canal10,11 Compared to middle ear surgery:<br />
• Safe and reliable means<br />
of restoring hearing<br />
• A reversible intervention<br />
• No risk of additional<br />
hearing impairment<br />
• The <strong>Baha</strong> can be evaluated<br />
prior to surgery
PaRT 1: identifying candidates<br />
PART 1 Identifying candidates<br />
There are three main audiological indications for the <strong>Baha</strong> ® System :<br />
• Conductive hearing loss<br />
• Mixed hearing loss<br />
• Single-sided sensorineural deafness (SSD)<br />
For each type of hearing loss there are specific criteria that will indicate who<br />
is a <strong>Baha</strong> candidate. There are also a range of other medical indications that may<br />
identify an individual as a <strong>Baha</strong> candidate. For details please see page 10.<br />
Conductive hearing loss<br />
Most candidates with a conductive hearing loss will benefit from <strong>Baha</strong>. As <strong>Baha</strong> sends<br />
sound directly to the cochlea via bone conduction, the conductive element of the hearing<br />
loss is effectively bypassed. This means that very little amplification is required.<br />
6 7<br />
Criteria:<br />
Size of conductive hearing loss<br />
Studies suggest that candidates with an air-bone gap of more than 30 dB (PTA 4 )<br />
will experience significant advantages with <strong>Baha</strong> compared to an air conduction<br />
(AC) hearing aid. 1-6<br />
Hearing Level (dB HL)<br />
-10<br />
0<br />
10<br />
20<br />
30<br />
40<br />
50<br />
60<br />
70<br />
80<br />
90<br />
100<br />
110<br />
120<br />
125<br />
Conductive hearing loss<br />
Frequency (Hz)<br />
250 500 1K 2K 4K 8K<br />
750 1.5K 3K 6K<br />
PaRT 1: identifying candidates<br />
Possible causes of<br />
conductive loss:<br />
• Cholesteatoma<br />
• Chronic otitis media<br />
• Congenital aural atresia<br />
• External otitis<br />
• Genetic causes<br />
• Ossicular disease<br />
• Other middle ear<br />
dysfunctions/diseases<br />
• Otosclerosis
PaRT 1: identifying candidates<br />
Possible causes<br />
of mixed loss:<br />
Mixed loss refers to a hearing loss<br />
that has both conductive and<br />
sensorineural elements. The<br />
sensorineural element of a<br />
hearing loss can stem from:<br />
• <strong>Cochlear</strong> otosclerosis<br />
• Disease related factors<br />
• Genetic causes<br />
• Noise trauma<br />
• Ototoxicity<br />
• Presbycusis<br />
For additional etiologies, see also<br />
Possible causes of conductive loss,<br />
page 7 and Medical indications,<br />
page 10.<br />
Mixed hearing loss<br />
Many individuals with mixed hearing loss are suitable candidates. <strong>Baha</strong>® sends sound<br />
directly to the cochlea via bone conduction, bypassing the conductive element of<br />
the hearing loss and providing amplification to compensate for the sensorineural<br />
component of the hearing loss.<br />
Criteria:<br />
the air-bone gap<br />
The air-bone gap is a good indicator of how suitable <strong>Baha</strong> will be for a candidate.<br />
The greater the air-bone gap, the more the candidate will benefit from <strong>Baha</strong>. Studies<br />
suggest that candidates with an air-bone gap of more than 30 dB (PTA 4 ) will benefit<br />
more from <strong>Baha</strong> than from a hearing aid. 1-6<br />
Extent of the sensorineural hearing loss<br />
Patients with a mild-to-moderate sensorineural component to their hearing loss<br />
are suitable candidates. The <strong>Baha</strong> Sound Processor can compensate for some degree<br />
of the sensorineural loss but, as the conductive part of the loss is bypassed, little<br />
amplification is required. Compared to conventional hearing aids, the <strong>Baha</strong> uses much<br />
less amplification. The most powerful <strong>Baha</strong> Sound Processor makes it possible to<br />
compensate for a sensorineural element of up to 65 dB HL (averaged across 500,<br />
1000, 2000, 3000 Hz) in a mixed hearing loss. For more information, please see the<br />
section on Device selection, page 21.<br />
Hearing Level (dB HL)<br />
-10<br />
0<br />
10<br />
20<br />
30<br />
40<br />
50<br />
60<br />
70<br />
80<br />
90<br />
100<br />
110<br />
120<br />
125<br />
Mixed hearing loss<br />
Frequency (Hz)<br />
250 500 1K 2K 4K 8K<br />
750 1.5K 3K 6K<br />
Single-sided deafness (SSD)<br />
<strong>Candidate</strong>s with SSD and normal hearing in the good ear will benefit from <strong>Baha</strong>. 12<br />
The <strong>Baha</strong> Sound Processor picks up sound on the deaf side and sends it via bone conduction to<br />
the contralateral intact cochlea to overcome the head shadow effect, which leads to improved<br />
speech understanding and 360° sound awareness. 7-9<br />
8 9<br />
Criteria:<br />
normal hearing in the good ear<br />
<strong>Candidate</strong>s must have normal hearing in the good ear defined as thresholds of less than or<br />
equal to 20 dB HL (averaged across 500, 1000, 2000, and 3000 Hz). If a patient later develops<br />
some hearing loss in the good ear, fitting of a more powerful <strong>Baha</strong> Sound Processor may be<br />
useful to supply needed amplification.<br />
<strong>Candidate</strong> motivation<br />
As SSD patients may have specific expectations due to their type of hearing loss, it is important<br />
that their expectations are realistic and that they perceive hearing from the deaf side as a need.<br />
Hearing Level (dB HL)<br />
-10<br />
0<br />
10<br />
20<br />
30<br />
40<br />
50<br />
60<br />
70<br />
80<br />
90<br />
100<br />
110<br />
120<br />
125<br />
Single-sided deafness (SSD)<br />
Frequency (Hz)<br />
250 500 1K 2K 4K 8K<br />
750 1.5K 3K 6K<br />
PaRT 1: identifying candidates<br />
Possible causes of<br />
single-sided deafness:<br />
• Acoustic neuroma tumors<br />
• Genetic causes<br />
• Ménière’s disease<br />
• Neurological<br />
degenerative disease<br />
• Ototoxic drugs<br />
• Sudden deafness<br />
• Surgical interventions<br />
• Trauma<br />
advantages of <strong>Baha</strong><br />
Compared to CRoS aid:<br />
• No occlusion of the hearing ear<br />
• No need for cables to transmit<br />
sound from the deaf side<br />
• Better sound quality
PaRT 1: identifying candidates<br />
advantages of <strong>Baha</strong> ®<br />
Compared to conventional<br />
bone conduction hearing aids:<br />
• Direct bone conduction<br />
• Better amplification – no<br />
weakening of the signal as it<br />
passes through skin<br />
• Superior sound quality<br />
• Improved comfort – no constant<br />
pressure to the skull<br />
• Discretion and improved<br />
cosmetic appearance13,14,15,16 Compared to middle ear surgery:<br />
• Safe and reliable means<br />
of restoring hearing<br />
• A reversible intervention<br />
• No risk of additional<br />
hearing impairment<br />
• Results can be evaluated<br />
prior to surgery<br />
Medical indications<br />
Besides the type and degree of hearing loss, there are several medical indications that<br />
identify an individual as a potential candidate for <strong>Baha</strong>. These indications are:<br />
Skin allergies<br />
Patient allergies may be aggravated by the placement of an ear mold. A <strong>Baha</strong> device<br />
maintains an open ear canal.<br />
Congenital malformations<br />
For most candidates with congenital ear malformation, surgical intervention or a<br />
conventional bone-conduction hearing aid is often prescribed because an AC hearing<br />
aid is simply not an option. <strong>Baha</strong> has several advantages over conventional BC hearing<br />
aids and, compared to surgical reconstruction, the <strong>Baha</strong> System provides a reliable<br />
and cost efficient solution. 13,14 In cases where an auricular prosthesis or surgical<br />
reconstruction is planned, the position of the <strong>Baha</strong> Implant in relation to these<br />
procedures should be considered.<br />
Draining ears<br />
One common problem for otologists when treating candidates with middle ear<br />
disease is getting a dry ear with good hearing. If the candidate uses an AC hearing aid,<br />
the ear mold in the ear canal will aggravate the condition. When using the<br />
<strong>Baha</strong> System, the ear canal is left open, thus allowing the ear to dry. 1<br />
Ear canal stenosis<br />
Individuals with stenosis of the ear canal are not suitable for surgical intervention,<br />
and the use of conventional hearing aids can be difficult when fitting an ear mold.<br />
With <strong>Baha</strong>, the ear canal is bypassed using Direct Bone Conduction.<br />
Previous ear surgery<br />
<strong>Candidate</strong>s who have had previous surgeries using, for example, a canal wall down<br />
technique, may find it difficult to wear an ear mold without feedback problems.<br />
As no ear mold is required, <strong>Baha</strong> is a good solution.<br />
Radical cavity<br />
Individuals treated for chronic mastoiditis with a radical cavity may be precluded from<br />
the use of a conventional AC aid because such aids may occlude the ear canal thus<br />
aggravating the condition. The <strong>Baha</strong> System allows the ear canal to be left open.<br />
Syndromic hearing losses<br />
Individuals with syndromes such as Downs, 15 Goldenhar 17 and Treacher Collins 18<br />
can be suitable candidates for <strong>Baha</strong>. Treatment of these individuals often requires<br />
special consideration and counseling. A personal counseling plan that considers the<br />
type of syndrome, the severity of the condition, and general abilities is suggested.<br />
For these candidates, parents or caregivers will often take an active role in the care<br />
of the sound processor, abutment and abutment area, and they will need special<br />
instructions early on in the candidate selection process. 1<br />
PART 2 <strong>Candidate</strong> evaluation<br />
PaRT 2: <strong>Candidate</strong> evaluation<br />
In addition to the audiological evaluations, the candidate should have the opportunity<br />
to listen to a <strong>Baha</strong> Sound Processor. Several <strong>Baha</strong> products can be used for this purpose:<br />
test rod, testband, headband, and <strong>Baha</strong> Softband. The main difference between these<br />
products is that the testband and test rod are for short-term testing, while the<br />
headband and <strong>Baha</strong> Softband are for longer trials.<br />
10 11
PaRT 2: <strong>Candidate</strong> evaluation<br />
Recommended<br />
audiological tests:<br />
• Pure tone audiometry (average<br />
bone thresholds at 500, 1000,<br />
2000, and 3000 Hz) 19<br />
• Speech audiometry with PB word<br />
lists/HINT/QuikSIN (for instance,<br />
maximum speech intelligibility)<br />
• Sound field testing (<strong>Baha</strong>® device<br />
on a testband, or a <strong>Baha</strong> Softband)<br />
Practical points<br />
to consider:<br />
• Manual dexterity<br />
• Cosmetic aspects<br />
• Driving (if the candidate is a taxi<br />
driver, then the side facing the<br />
passenger is a good alternative)<br />
• Telephone use (if the candidate<br />
uses the telephone frequently, the<br />
opposite side to the “writing hand”<br />
may be the best choice)<br />
Adult candidates<br />
The <strong>Baha</strong> System works independently of the severity of the conductive part of the hearing<br />
loss because sound bypasses the outer and middle ear. The bone conduction threshold<br />
is therefore the most relevant measurement in the audiological assessment. Use the<br />
candidate’s air-bone gap as a guide to the benefits that can be expected from choosing <strong>Baha</strong><br />
instead of an AC hearing aid. Comparing the results of speech measurements in sound field,<br />
with and without the sound processor, will also be useful.<br />
Sound field testing of a <strong>Baha</strong> Sound Processor allows the candidate to hear the sound<br />
of a <strong>Baha</strong> device before surgery. For a realistic experience, allow the candidate to test a<br />
sound processor in different sound environments (for example by taking a walk around<br />
the hospital/clinic or surrounding area). For candidates with SSD, a longer trial, which allows<br />
testing of a <strong>Baha</strong> Sound Processor at home or work, is crucial.<br />
nOTe: In candidates with bone defects or other problems where the testband/headband<br />
is not suitable, the <strong>Baha</strong> Softband may provide a better testing solution (see Listening<br />
with a <strong>Baha</strong> Softband, page 19).<br />
<strong>Selection</strong> of implant side<br />
Bilateral fitting<br />
For candidates with binaural hearing loss, a bilateral fitting of <strong>Baha</strong>, which may lead to<br />
binaural hearing, should be considered as this improves speech understanding, sound<br />
localization, and general candidate satisfaction. 20-22 For bilateral fittings, bone conduction<br />
thresholds must be symmetrical (defined as less than 10 dB difference on average (PTA 4 )<br />
or less than 15 dB at individual frequencies).<br />
unilateral fitting<br />
For SSD, implantation is made on the deaf side. For conductive or mixed losses the general<br />
recommendation is to choose the side with the best cochlear function (the best bone<br />
conduction thresholds). The side the candidate perceives as having the greatest handicap<br />
should, however, be taken into account.<br />
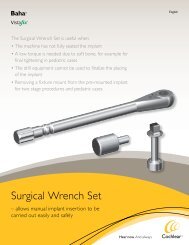
Listening with a <strong>Baha</strong> Testband<br />
1. Attach the sound processor to the plastic snap connector disc<br />
on the testband.<br />
2. Test that the <strong>Baha</strong> Sound Processor works by putting on the<br />
testband, plugging your ears and introducing sound.<br />
3. Put the testband on the candidate’s head placing the plastic snap<br />
connector disc against the selected mastoid.<br />
4. Position the sound processor behind the ear. To avoid feedback,<br />
make sure the processor doesn’t touch the ear or skin.<br />
Sound processor considerations<br />
Due to weakening of the sound signal as it passes through skin (attenuation),<br />
the gain from a <strong>Baha</strong> device is reduced by 2-15 dB* during sound-field testing<br />
compared to a sound processor fitted to an osseointegrated implant. 23,24<br />
Therefore, we recommend using a stronger processor for the test than the<br />
candidate’s audiogram would indicate. A stronger processor is most noticeable<br />
at higher frequencies because higher frequencies are weakened to a greater<br />
extent than low frequency signals. 25 For SSD, use a head worn sound processor.<br />
A body worn device will not help alleviate the head shadow effect due to its<br />
microphone placement.<br />
The new <strong>Baha</strong> Fitting software offers features such as BC Select and BC Direct<br />
that may help to optimize a <strong>Baha</strong> 3 Sound Processor demonstration with a<br />
headband or a <strong>Baha</strong> Softband.<br />
*Depending on the patient and the frequency, sound is weakened by 2-15 dB as it passes through skin.<br />
PaRT 2: <strong>Candidate</strong> evaluation<br />
12 13<br />
1<br />
2<br />
3<br />
4
PaRT 3: Counseling<br />
PART 3 Counseling<br />
Before they are treated, candidates should be motivated, well informed and counseled<br />
to have realistic expectations. <strong>Baha</strong> ® Counseling tools will be helpful for these purposes.<br />
The main points that should be covered during counseling are:<br />
• Benefits of <strong>Baha</strong> to the patient<br />
• The process of getting <strong>Baha</strong><br />
• Expectations<br />
• Aftercare<br />
• Reimbursement/funding<br />
PART 3:<br />
Benefits of <strong>Baha</strong> for the patient<br />
Conductive/mixed hearing loss<br />
The use of direct bone conduction to transmit sound gives <strong>Baha</strong> several unique advantages<br />
over other treatments for conductive/mixed hearing loss.<br />
The most notable benefits of <strong>Baha</strong> for a candidate with conductive or mixed hearing loss,<br />
compared to conventional hearing aids, are:<br />
• Need for less amplification as the conductive element of the hearing loss is bypassed<br />
• No occlusion of the ear canal<br />
• Excellent sound quality as very little amplification is required<br />
When compared to middle ear surgery <strong>Baha</strong> will provide:<br />
• A safe and reliable way to restore the candidate’s hearing<br />
• No risk of additional hearing impairment<br />
• A reversible intervention<br />
• The opportunity to test the <strong>Baha</strong> before surgery is performed<br />
In comparison to conventional bone conduction hearing aids <strong>Baha</strong> will give the candidate:<br />
• Better sound quality due to direct bone conduction<br />
• Increased wearing comfort, as there is no constant pressure to the skull<br />
If the candidate has frequent ear infections <strong>Baha</strong> can provide:<br />
• Reduced incidence<br />
• A dryer ear canal as the ear canal is left open<br />
SSD<br />
As SSD candidates may have specific expectations due to their type of hearing loss, it is<br />
important to ensure that these expectations are realistic. The audiologist or physician can<br />
help the patients to understand their perceived handicap, and more importantly, their<br />
motivation for hearing.<br />
nOTe: Restoration of directional hearing should not be expected after fitting as all<br />
sounds will be processed by the remaining functioning cochlea. 8 Some patients, however,<br />
report a rudimentary form of directional hearing resulting from a difference in the<br />
perceived quality of the <strong>Baha</strong> processed sound.<br />
For candidates with SSD, <strong>Baha</strong> provides several benefits when compared<br />
to a conventional CROS aid:<br />
• No occlusion of the hearing ear<br />
• No need for cables to transmit sound from the deaf side<br />
• Better sound quality<br />
• Only one device is worn, versus two with the CROS aid<br />
PaRT 3: Counseling<br />
14 15
PaRT 3: Counseling<br />
The process of getting <strong>Baha</strong> ®<br />
Review the process of <strong>Baha</strong> treatment with the candidate:<br />
• Inform the candidate about the different audiological evaluations that will be performed.<br />
• Tell the candidate that they will need to have surgery. Emphasize that the surgical<br />
procedure is considered minor and may be performed in an outpatient setting under local or<br />
general anesthetic.<br />
• Explain that a small titanium implant will be placed just behind the chosen ear. Clarify that<br />
the implant will be connected to an abutment and that it is the abutment that will protrude<br />
through the skin. At this point showing an actual implant and abutment may reduce the<br />
candidate’s anxiety.<br />
• Tell the candidate that after surgery they will have a small hair-free area around the<br />
abutment and that they may experience some numbness in that area. The numbness may<br />
or may not pass with time.<br />
• Inform the candidate that they will have a dressing and pressure bandage over the<br />
abutment when they come from surgery and that the dressing will be changed (5-7 days<br />
post-operatively) and removed (10-14 days post-operatively).<br />
•<br />
Explain how long the implant will take to fully osseointegrate (usually up to 3 months)<br />
and how the sound processor will be fitted.<br />
nOTe: Emphasize that there is no risk of further damage to the candidate’s hearing from <strong>Baha</strong><br />
surgery. More detailed information on the surgical procedure should be provided by the surgeon.<br />
Expectations<br />
Ensure the candidate has realistic expectations. Preoperative testing is essential for keeping<br />
candidate expectations reasonable. Listening to a <strong>Baha</strong> Sound Processor on a testband/<strong>Baha</strong><br />
Softband provides a practical experience close to that of the post-surgical outcome In this<br />
context, it is important to note that true directionality will not be restored for SSD candidates.<br />
Aftercare<br />
<strong>Candidate</strong>s must be able to maintain and clean the area around the abutment (either<br />
themselves or with help from others). Careful consideration must be given to the candidate’s<br />
ability to maintain proper hygiene. With children, responsibility for maintaining hygiene falls<br />
on the parents or caregivers.<br />
Reimbursement and funding<br />
PART 4 Pediatric candidacy<br />
Patient selection<br />
The <strong>Baha</strong> Sound Processor can be fitted to infants and children in need of amplification<br />
via bone conduction. The indications for a <strong>Baha</strong> device are generally the same as for<br />
adults, except in the US and Canada, <strong>Baha</strong> implantation is indicated for children five<br />
years of age and older. Younger children may be fitted with a <strong>Baha</strong> using the Softband.<br />
PaRT 4: Pediatric candidacy<br />
16<br />
As reimbursement for <strong>Baha</strong> is an important factor for the candidate, this should be discussed<br />
during the preoperative evaluation. Terms and conditions of reimbursement and funding for<br />
<strong>Baha</strong> differ from area to area. For information about the terms and conditions applicable in<br />
your area, please consult your local <strong>Cochlear</strong> representative. In the U.S.A., please refer to<br />
the <strong>Baha</strong> reimbursement guide.<br />
17
PaRT 4: Pediatric candidacy<br />
use age appropriate<br />
tests to evaluate<br />
audibility and speech<br />
understanding:<br />
• Auditory Brainstem Response<br />
(ABR): Infants<br />
• Auditory Steady State Response<br />
(ASSR): Infants<br />
• Otoacoustic Emission (OAE):<br />
Infants (requires normal middle<br />
ear function)<br />
• Behavioral Observational<br />
Audiometry (BOA):<br />
Infants from 7-8 months<br />
• Visual Reinforcement Audiometry<br />
(VRA): Children from about six<br />
months up to 2-3 years<br />
• Play audiometry: Children<br />
between 3-5 years of age *<br />
• Listening with a <strong>Baha</strong>® Softband<br />
* Play audiometry can be done with<br />
warble tones, speech or animal sounds.<br />
Evaluation<br />
As in an adult patient evaluation, the bone conduction threshold is the most relevant in<br />
the audiological assessment. Use the air-bone gap as a guide to the benefits that can be<br />
expected from choosing the <strong>Baha</strong> System. There may also be medical indications why <strong>Baha</strong><br />
will be the solution of choice for the child. If possible, obtain speech measurements in the<br />
sound field with and without the sound processor.<br />
We recommend fitting infants and children who are too young or not ready for implantation<br />
with the <strong>Baha</strong> Softband. This will instantly improve the child’s hearing and is a very good<br />
introduction to the advantages of <strong>Baha</strong>, both for the child and for the parents/caregivers.<br />
The decision to implant the child can then be postponed to a later date and is usually easy,<br />
once the benefits to the child have been observed.<br />
<strong>Selection</strong> of implant side<br />
Clinical research suggests that children with binaural conductive hearing loss should be<br />
fitted with bilateral <strong>Baha</strong> Sound Processors on a <strong>Baha</strong> Softband preferably before the age of<br />
6 months. 1 If bilateral fitting is contraindicated, fit the side with the best bone conduction<br />
thresholds and skull thickness. For children with SSD, the <strong>Baha</strong> Sound Processor is placed<br />
on the deaf side.<br />
Counseling<br />
Parents of hearing-impaired children will have a great need for counseling. Parents may<br />
have questions about the hearing loss and how it will affect their child’s development. They<br />
need information on how to help their child achieve the best possible results, especially in<br />
speech and language development. They will want to know why <strong>Baha</strong> is the best solution<br />
for their child. In addition, counseling should cover the <strong>Baha</strong> treatment process from both<br />
a short- and long-term perspective. Therefore, both <strong>Baha</strong> Softband and surgery should<br />
be discussed.<br />
Device selection<br />
The <strong>Baha</strong> Softband is a preoperative hearing solution and does not provide the full benefits<br />
of a sound processor connected to an implant (see page 13). This must be taken into<br />
consideration when choosing an appropriate sound processor.<br />
CauTiOn: the older <strong>Baha</strong> Softband contain natural rubber latex<br />
that may cause allergic reactions. the newer generation<br />
<strong>Baha</strong> Softbands are latex free.<br />
Listening with a <strong>Baha</strong> Softband<br />
Try to make the first moments with the <strong>Baha</strong> Softband as pleasant for the child as possible.<br />
It is very important that the child has positive associations with using the <strong>Baha</strong> Softband.<br />
1. Program the sound processor for patient’s individual bone line using the <strong>Baha</strong> Fitting<br />
Software. Optimize the sound processor fitting for use with <strong>Baha</strong> Softband by selecting<br />
suitable parameters in the BC Select screen. Also, whenever possible, conduct BC Direct<br />
measurements, which are in-situ bone conduction thresholds, using patient’s processor.<br />
2. Attach the sound processor to the plastic snap connector disc on the <strong>Baha</strong> Softband.<br />
3. Test that the <strong>Baha</strong> Softband works by putting it on yourself, plugging your ears<br />
and introducing sound.<br />
4. Put the <strong>Baha</strong> Softband around the child’s head, quite loosely at first.<br />
5. Place the plastic snap connector disc against the mastoid or another bony location<br />
of the skull. Avoid placing it on the temple bone, as this may be uncomfortable.<br />
Check that the entire snap connector disc is in contact with the skull bone. Turn on<br />
the sound processor.<br />
6. Tighten the <strong>Baha</strong> Softband until it is close-fitting enough to ensure effective sound<br />
transmission but loose enough not to cause the child any discomfort.<br />
7. Have the parent or caregiver talk to the child, sing a song, or another pleasant sounding<br />
experience. Watch for the child’s reaction.<br />
TiP: Make sure your finger fits between the skull and <strong>Baha</strong> Softband – this will ensure<br />
that the <strong>Baha</strong> Softband is not too tight.<br />
nOTe: Once the <strong>Baha</strong> Softband is tight enough to transmit sound effectively,<br />
additional tightening will only increase the sound marginally.<br />
Additional considerations<br />
Early amplification<br />
Early access to amplification is crucial for a child’s speech, language and educational<br />
development. Yoshinaga-Itano reports that children who receive hearing rehabilitation<br />
before the age of 6 months perform significantly better on language tests at the age of<br />
3 to 4 years than do children fitted later in life. 26 The Yoshinaga-Itano study concludes<br />
that a delay in intervention may lead to a permanent language deficit.<br />
PaRT 4: Pediatric candidacy<br />
Recommended age for implantation<br />
Implant placement must wait until the child has sufficient bone volume and bone<br />
quality. This can vary from child to child but, based on studies, the child should<br />
have a skull bone at least 2.5 mm thick.<br />
18 19<br />
27,28,29 Note in the US and Canada, the<br />
<strong>Baha</strong> implant is indicated for children five years of age or older. Younger children can<br />
5<br />
use a <strong>Baha</strong> sound processor on a Softband.<br />
2<br />
3<br />
4
PaRT 5: Device consideration<br />
PART 5 Device considerations<br />
When calculating the amplification needs of a <strong>Baha</strong> ® candidate, the bone conduction thresholds in<br />
the audiogram provide the most important information. The <strong>Baha</strong> Sound Processor will have to<br />
produce sufficient power to compensate for any sensorineural element to the hearing loss. To<br />
help your candidate select the correct sound processor, follow these guidelines. Please note that<br />
the new generation <strong>Baha</strong> 3 Sound Processors are programmable. The factory setting may be<br />
a starting point for a quick demonstration in some cases but it is suggested that a processor is<br />
custom programmed using <strong>Baha</strong> Fitting Software for the best candidate experience.<br />
Device selection based on hearing loss type<br />
Conductive hearing loss<br />
For candidates with a purely conductive loss, we recommend focusing on which sound<br />
processor has the most useful features for the candidate. Any <strong>Baha</strong> device will provide<br />
sufficient amplification.<br />
Mixed hearing loss<br />
The fitting range of the selected sound processor must cover the size of the sensorineural<br />
loss as the device will need to compensate for the degree of sensorineural impairment.<br />
Similar to other hearing devices, the clinical rule of thumb is: if the hearing loss is in the<br />
lower third of the fitting range, a more powerful sound processor may result in better<br />
outcomes for the candidate. Providing a second device for situations where more power<br />
is required could also be considered.<br />
SSD<br />
For most candidates with SSD, the choice of sound processor can be based on which device<br />
has the most useful features. In some cases, however, the sound processor may need to<br />
deliver added amplification to provide sufficient audibility to the contralateral ear.<br />
SSD candidates may benefit from a more powerful head worn <strong>Baha</strong> in the following situations:<br />
• Larger than expected interaural attenuation. Extra amplification may be required to<br />
ensure audibility in the good ear.<br />
• Sensorineural hearing loss developing in the ‘normal’ ear over time for instance due to<br />
presbycusis or noise exposure. Extra gain may be required to amplify the sound above<br />
the candidate’s thresholds.<br />
To evaluate the benefit of <strong>Baha</strong> for SSD candidates, a longer trial or testing – that occurs<br />
outside of the sound booth – is crucial. Usually a two-week trial will provide a good<br />
indication of what the candidates may expect from <strong>Baha</strong>.<br />
nOTe: Due to weakening of the sound signal as it passes through the skin, the gain<br />
from a <strong>Baha</strong> Sound Processor will be reduced by 2-15 dB during demonstration on a<br />
Softband or Headband. Therefore, we recommend using the most powerful head worn<br />
device for this process.<br />
PaRT 5: Device consideration<br />
20 21
PaRT 5: Device consideration<br />
Additional considerations for device selection<br />
• Improved clarity of speech in difficult listening situations<br />
A sound processor with directional microphones will prioritize sounds coming<br />
from the front versus sounds coming from behind, which may make it easier<br />
to hear speech in noise.<br />
• Better comfort in noisy listening situations<br />
Directional microphones provide less gain for lower pitched sounds which may<br />
making it easier to hear in noisy situations. In addition, a directional microphone<br />
prioritizes sounds from the front versus those from behind, which may improve speech<br />
understanding in noise.<br />
• Improved audibility in difficult listening situations<br />
There may be situations where additional audibility is needed. A more powerful<br />
<strong>Baha</strong>® device may make sounds (especially those in the higher frequencies, e.g.,<br />
‘s’ and ‘sh’) easier to understand. A <strong>Baha</strong> with a specific noise program helps<br />
ensure audibility and comfort.<br />
• Listening from a distance<br />
A more powerful sound processor will amplify soft sounds more so they may become<br />
more audible. This may enable better hearing from a distance (e.g., in church).<br />
• Music appreciation<br />
A sound processor with a Music Program provides a flatter frequency response which is<br />
best for enjoying music.<br />
Benefits of providing different programs<br />
within the sound processor<br />
Each program within the programmable sound processors may provide different<br />
performance advantages, depending on the specific listening environment. Therefore, some<br />
candidates may benefit from having different listening programs. This gives the candidate<br />
the unique opportunity to select the best listening program for a given situation.<br />
PART 6 Case histories<br />
Patient: Male<br />
age: 36<br />
occupation: Salesman<br />
type of hearing loss: Unilateral mixed hearing loss<br />
Diagnosis: Congenital facial paraesthesia and<br />
malformation of outer and middle ear<br />
aided side: Left<br />
unaided audiogram:<br />
Frequency(Hz)<br />
History: The patient received a Vistafix ear prosthesis in his<br />
late teens and was later fitted with a <strong>Baha</strong> device in 2006.<br />
He had never used a hearing device before. The benefits of<br />
<strong>Baha</strong> have been many and the patient considers it a useful<br />
solution for his hearing loss.<br />
Pta 4 improvement: 64 to 26 dB HL<br />
22 23<br />
Hearing Level (dB HL)<br />
Hearing Level (dB HL)<br />
-10<br />
0<br />
10<br />
20<br />
30<br />
40<br />
50<br />
60<br />
70<br />
80<br />
90<br />
100<br />
110<br />
120<br />
125<br />
Frequency (Hz)<br />
250 500 1K 2K 4K 8K 125<br />
750 1.5K 3K 6K<br />
-10<br />
0<br />
10<br />
20<br />
30<br />
40<br />
50<br />
60<br />
70<br />
80<br />
90<br />
100<br />
110<br />
120<br />
Hearing Level (dB HL)<br />
aided audiogram:<br />
Frequency (Hz)<br />
250 500 1K 2K 4K 8K<br />
750 1.5K 3K 6K<br />
B = Aided threshold with <strong>Baha</strong> in soundfield testing<br />
PaRT 6: Case histories
PaRT 6: Case histories<br />
Patient: Female<br />
age: 46<br />
occupation: Homemaker<br />
type of hearing loss: Binaural conductive hearing loss<br />
Diagnosis: Treacher Collins syndrome<br />
aided side: Right<br />
Hearing Level (dB HL)<br />
-10<br />
0<br />
10<br />
20<br />
30<br />
40<br />
50<br />
60<br />
70<br />
80<br />
90<br />
100<br />
110<br />
120<br />
125<br />
unaided audiogram:<br />
Frequency (Hz)<br />
History: The patient received her first <strong>Baha</strong> ® 27 years<br />
ago and still uses the same implant. She changed the<br />
abutment to the snap coupling when she upgraded<br />
her <strong>Baha</strong> Sound Processor.<br />
Pta 4 improvement 71 to 21 dB HL<br />
250 500 1K 2K 4K 8K 125<br />
750 1.5K 3K 6K<br />
-10<br />
0<br />
10<br />
20<br />
30<br />
40<br />
50<br />
60<br />
70<br />
80<br />
90<br />
100<br />
110<br />
120<br />
aided audiogram:<br />
Frequency (Hz)<br />
250 500 1K 2K 4K 8K<br />
750 1.5K 3K 6K<br />
B = Aided threshold with <strong>Baha</strong> in soundfield testing<br />
Patient: Female<br />
age: 13<br />
occupation: Student<br />
type of hearing loss: Binaural Conductive hearing loss<br />
Diagnosis: Treacher Collins syndrome<br />
aided side: Left<br />
unaided audiogram:<br />
History: The patient has used <strong>Baha</strong> since she was a child.<br />
She experiences great benefit from the <strong>Baha</strong> in<br />
classroom situations.<br />
Pta 4 improvement: 54 to 20 dB HL<br />
aided audiogram:<br />
24 25<br />
Hearing Level (dB HL)<br />
-10<br />
0<br />
10<br />
20<br />
30<br />
40<br />
50<br />
60<br />
70<br />
80<br />
90<br />
100<br />
110<br />
120<br />
125<br />
Frequency (Hz)<br />
250 500 1K 2K 4K 8K<br />
750 1.5K 3K 6K<br />
Hearing Level (dB HL)<br />
-10<br />
0<br />
10<br />
20<br />
30<br />
40<br />
50<br />
60<br />
70<br />
80<br />
90<br />
100<br />
110<br />
120<br />
125<br />
Frequency (Hz)<br />
250 500 1K 2K 4K 8K<br />
750 1.5K 3K 6K<br />
B = Aided threshold with <strong>Baha</strong> in soundfield testing<br />
PaRT 6: Case histories
PaRT 6: Case histories<br />
Patient: Male<br />
age: 53<br />
type of hearing loss: Binaural mixed hearing loss<br />
occupation: Nurse<br />
Diagnosis: Chronic otitis media, middle ear<br />
bones removed after osteomyelitis, tympanic<br />
membranes ruptured bilaterally<br />
aided side: Right<br />
Hearing Level (dB HL)<br />
-10<br />
0<br />
10<br />
20<br />
30<br />
40<br />
50<br />
60<br />
70<br />
80<br />
90<br />
100<br />
110<br />
120<br />
125<br />
unaided audiogram: aided audiogram:<br />
Frequency (Hz)<br />
250 500 1K 2K 4K 8K 125<br />
750 1.5K 3K 6K<br />
-10<br />
0<br />
10<br />
20<br />
30<br />
40<br />
50<br />
60<br />
70<br />
80<br />
90<br />
100<br />
110<br />
120<br />
History: The patient has had hearing problems his entire life.<br />
The patient received his <strong>Baha</strong> ® in 2004. In 2007 he received a<br />
new implant after losing the original due to trauma. He uses<br />
his <strong>Baha</strong> constantly and is extremely pleased with the sound.<br />
Pta 4 improvement: 85 to 24 dB HL<br />
Hearing Level (dB HL)<br />
Frequency (Hz)<br />
250 500 1K 2K 4K 8K<br />
750 1.5K 3K 6K<br />
B = Aided threshold with <strong>Baha</strong> in soundfield testing<br />
Patient: Male<br />
age: 52<br />
type of hearing loss: Single-sided deafness (SSD)<br />
occupation: Nurse<br />
Diagnosis: Acoustic Neuroma (AN) left ear<br />
AN surgery took place in 1998<br />
aided side: Left<br />
unaided audiogram:<br />
History: The patient was offered a CROS aid following<br />
acoustic neuroma surgery. He used the CROS aid for one<br />
month but felt more handicapped with it, than without it.<br />
An implant for the <strong>Baha</strong> System was placed in May 2003, and<br />
in August of that year, a <strong>Baha</strong> was fitted. At clinical follow-up<br />
one year later he reported using the <strong>Baha</strong> Sound Processor for<br />
14 hours a day, seven days a week.<br />
26 27<br />
Hearing Level (dB HL)<br />
-10<br />
0<br />
10<br />
20<br />
30<br />
40<br />
50<br />
60<br />
70<br />
80<br />
90<br />
100<br />
110<br />
120<br />
125<br />
Frequency (Hz)<br />
250 500 1K 2K 4K 8K<br />
750 1.5K 3K 6K<br />
Hearing Level (dB HL)<br />
Hearing Level (dB HL)<br />
-10<br />
0<br />
10<br />
20<br />
30<br />
40<br />
50<br />
60<br />
70<br />
80<br />
90<br />
100<br />
110<br />
120<br />
125<br />
aided Frequency(Hz) audiogram:<br />
Frequency (Hz)<br />
PaRT 6: Case histories<br />
250 500 1K 2K 4K 8K<br />
750 1.5K 3K 6K<br />
B = Aided threshold with <strong>Baha</strong> in soundfield testing
PaRT 7: Clinical results References<br />
PART 7 Clinical results<br />
The <strong>Baha</strong>® System has proven to be an effective hearing solution and several clinical studies demonstrate patient benefits.<br />
Mixed/conductive hearing loss<br />
“The <strong>Baha</strong> provides a reliable and predictable adjunct for auditory rehabilitation in appropriately selected patients, offering a<br />
means of dramatically improving hearing thresholds in patients with conductive or mixed hearing loss who are otherwise unable<br />
to benefit from traditional hearing aids.” 6<br />
“It can be stated that patients with an acquired unilateral air-bone gap benefited from using the <strong>Baha</strong>. This was not only reflected<br />
in the audiological results, but also in the patients’ opinions.” 30<br />
SSD<br />
“Subjects found <strong>Baha</strong> amplification to be consistently more useful [compared to CROS] in a variety of listening environments<br />
experienced in daily life. On HINT testing the <strong>Baha</strong> provided clinically significant benefit in several noise conditions.” 31<br />
“The speech-in-noise measurements demonstrated the efficacy of the <strong>Baha</strong> [...] to lift the head shadow.<br />
patients were still satisfied at 1-year follow-up, according to the four questionnaires*. ” 8<br />
Pediatric<br />
“Bone-anchored hearing aids provide an exceptionally effective method of rehabilitating the child with conductive hearing loss<br />
or inability to wear AC aids due to chronic otorrhea.” 29<br />
“The <strong>Baha</strong> is an effective hearing aid for children with congenital hearing loss, whether they were previous air-conduction<br />
or bone-conduction aid wearers. The majority was overall more satisfied with their <strong>Baha</strong> than their previous aid.” 17<br />
“Fixture survival rates equivalent to those seen in an adult population. Also significant improvements seen in aided<br />
thresholds with <strong>Baha</strong>s demonstrate the safety and efficacy of the <strong>Baha</strong>.” 16<br />
* The Abbreviated Profile of Hearing Aid Benefit, the Glasgow Hearing Aid Benefit Profile,<br />
the International Outcome Inventory for Hearing Aids, and the Single-Sided Deafness questionnaire.<br />
References<br />
1. Snik AF, Mylanus EA, Proops DW, Wolfaardt J, Hodgetts WA, Somers T, Niparko JK,<br />
Wazen JJ, Sterkers O, Cremers CW, Tjellström A. Consensus statements on the <strong>Baha</strong><br />
system: where do we stand at present? The Annals of Otology, Rhinology &<br />
Laryngology 2005 Dec;114(195):1-12.<br />
2. Hol MK, Snik AF, Mylanus EA, Cremers CW. Long-term results of bone-anchored hearing<br />
aid recipients who had previously used air-conduction hearing aids. Archives of<br />
Otolaryngology-Head & Neck Surgery 2005 Apr;131(4):321-5.<br />
3. McDermott AL, Dutt SN, Reid AP, Proops DW. An intra-individual comparison of the<br />
previous conventional hearing aid with the bone-anchored hearing aid: The Nijmegen<br />
group questionnaire. The Journal of Laryngology and Otology 2002 Jun;116 Suppl 28:15-9.<br />
4. Mylanus EA, Snik AF, Cremers CW. Patients’ opinions of bone-anchored vs. conventional<br />
hearing aids. Archives of Otolaryngology-Head & Neck Surgery.1995 Apr;121(4):421-5.<br />
5. Mylanus EA, van der Pouw KC, Snik AF, Cremers CW. Intra-individual comparison of the<br />
bone-anchored hearing aid and air-conduction hearing aids. Archives of Otolaryngology-<br />
Head & Neck Surgery 1998;124(3):271-6.<br />
6. Lustig LR, Arts HA, Brackmann DE, et al. Hearing rehabilitation using the <strong>Baha</strong><br />
bone-anchored hearing aid: results in 40 patients. Otology & Neurotology<br />
2001;22(3):328-34.<br />
7. Wazen JJ, Spitzer JB, Ghossaini SN, Fayad JN, Niparko JK, Cox K, et al. Transcranial<br />
contralateral cochlear stimulation in unilateral deafness. Otolaryngology-Head & Neck<br />
Surgery 2003;129(3):248-54.<br />
8. Hol MK, Bosman AJ, Snik AF, Mylanus EA, Cremers CW. Bone-anchored hearing aids in<br />
unilateral inner ear deafness: an evaluation of audiometric and patient outcome<br />
measurements. Otology & Neurotology 2005 Sep;26(5):999-1006.<br />
9. Bosman AJ, Hol MKS,Snik AFM,.Mylanus EAM Cremers CWRJ, Bone-anchored hearing<br />
aids in unilateral inner ear deafness. Acta Oto-Laryngologica 2003;123(2):258-260.<br />
10. Burell SP, Cooper HC, Proops DW. The bone-anchored hearing aid-the third option for<br />
otosclerosis. Journal of Laryngology and Otology 1996 Dec;110 Suppl 21:31-37.<br />
11. Snik AFM, Mylanus EAM, Creemers WRJ. The Bone-anchored hearing aid – A solution for<br />
previously unresolved otologic problems. The Otolaryngologic Clinics of North America<br />
2001;34(2):365-72.<br />
12. Lin LM, Bowditch s, Anderson MJ, May B, Cox K, Niparko JK. Amplification in the<br />
rehabilitation of unilateral deafness: speech in noise and directional hearing effects<br />
with bone-anchored hearing aids <strong>Baha</strong> Compact and Divino. Otology and Neurotology<br />
2006 Feb;27(2):172-82.<br />
13. Hol MK, Cremers CW, Coppens-Schellekens W, Snik AF. The <strong>Baha</strong> Softband. A new<br />
treatment for young children with bilateral congenital aural atresia. International Journal<br />
of Pediatric Otorhinolaryngology 2005 Jul;69(7):973-80.<br />
14. Evans A.K, Kazahaya K. Surgery or implantable hearing devices? The experts question<br />
revisited. International Journal of Pediatric Otorhinolaryngology 2007 Mar;71(3):367-374.<br />
15. Sheehan PZ, Hans PS. UK and Ireland experience of bone-anchored hearing aids (<strong>Baha</strong>) in<br />
individuals with Down syndrome. International Journal of Pediatric Otorhinolaryngology,<br />
2006 Jun;70(6):981-6.<br />
16. Tietzle L, Papsin B. Utilization of bone-anchored hearing aids in children. International<br />
Journal of Pediatric Otorhinolaryngology 2001 Apr;58(1):75-80.<br />
17. Powell RH, Burell SP, Cooper HR, Proops DW. The Birmingham bone-anchored hearing<br />
aid programme: Pediatric.experience and results. The Journal of Laryngology & Otology,<br />
1996;110:21-9.<br />
18. Marres HA, Cremers CW, Marres EH. The Treacher Collins syndrome. Management of<br />
major and minor ear anomailes. Revue de laryngologie otolologie rhinologie.<br />
1995:116, 2;105-108.<br />
19. Catlin FI. <strong>Guide</strong> for evaluation of hearing handicap. Otolaryngologic Clinics of North<br />
America. 1979 Aug: 12(3):655-663.<br />
20. Bosman AJ, Snik AF, van der Pouw CT, Mylanus EA, Cremers CW. Audiometric evaluation<br />
of bilaterally fitted bone-anchored hearing aids. Audiology 2001 May-Jun;40(3):158-67.<br />
21. Burrell SP, Cooper HR, Reid AP, Proops DW. Patient satisfaction with bilateral<br />
bone-anchored hearing aids: the Birmingham experience. Journal of Laryngology<br />
& Otology Suppl 2002 Jun 1;116 Suppl 28:37-46.<br />
22. Dutt SN, McDermott AL, Burrell SP, Cooper HR, Reid AP, Proops DW. Speech<br />
intelligibility with bilateral bone-anchored hearing aids: the Birmingham experience.<br />
The Journal of Laryngology & Otology 2002 Jun 1;116 Suppl 28:47-51.<br />
23. Håkansson B, Tjellström A., Rosenhall U. Hearing thresholds with direct bone<br />
conduction versus conventional bone conduction. Scandinavian Audiology<br />
1984;13(1):3-13.<br />
24. Gründer I, Seidl RO, Ernst A, Todt I. Relative value of <strong>Baha</strong> testing for the postoperative<br />
audiological outcome. HNO 2007 Sep 20.<br />
25. Eeg-Olofsson M. Transmission of bone conducted sound in the human skull measured<br />
by cochlear vibrations. Proceedings of the first International Symposium of Bone<br />
Conduction Hearing and Osseointegration; 2007 Jul 12-14; Halifax, Canada.<br />
26. Yoshinaga-Itano C. Early Intervention after universal neo-natal hearing screening:<br />
impact on outcomes. Mental Retardation and Developmental Disability Research<br />
Reviews 2003;9(4):252-66.<br />
27. Tjellström A, Håkansson B, Granström G, Bone-anchored hearing aids: current status in<br />
adults and children. Otolaryngologic Clinics of North America 2001 Apr;34(2):337-64.<br />
28. Davids T, Gordon KA, Clutton D, Papsin BC. Bone-anchored hearing aids in infants and<br />
children younger than 5 years. Archives of Otolaryngology-Head & Neck Surgery, 2007<br />
Jan;133(1):51-5.<br />
29. Papsin BC, Sirimanna TKS, Albert DM, Bailey M. Surgical experience with bone-anchored<br />
hearing aids in children. The Laryngoscope, 1997 Jun;107(6):801-6.<br />
30. Hol MKS, Snik AFM, Mylanus EAM, Cremers CWRJ . Does the bone-anchored hearing<br />
aid have a complimentary effect on audiological and subjective outcomes in candidates<br />
with unilateral conductive hearing loss?, Audiology & Neurotology 2005 May-Jun;<br />
10(3):159-68.<br />
31. Niparko JK, Cox KM, Lustig LR. Comparison of the bone-anchored hearing aid<br />
implantable hearing device with contralateral routing of offside signal amplification in<br />
the rehabilitation of unilateral deafness. Otology & Neurotology, 2003 Jan;24(1):73-78.<br />
28 29
notes<br />
Notes Notes<br />
30 31<br />
notes
this is the <strong>Cochlear</strong> promise to you. As the global leader<br />
in hearing solutions, <strong>Cochlear</strong> is dedicated to bringing the<br />
gift of sound to people all over the world. With our hearing<br />
solutions, <strong>Cochlear</strong> has reconnected over 250,000 cochlear<br />
implant and <strong>Baha</strong> ® recipients to their families, friends and<br />
communities in more than 100 countries.<br />
Along with the industry’s largest investment in research<br />
and development, we continue to partner with leading<br />
international researchers and hearing professionals, ensuring<br />
that we are at the forefront in the science of hearing.<br />
For patients receiving any <strong>Cochlear</strong> hearing system, our<br />
commitment is that for the rest of your life we will be<br />
here to support you.<br />
As your patient’s partner in hearing for life, <strong>Cochlear</strong> believes it is important to convey<br />
not only the benefits, but also the potential risks associated with a <strong>Baha</strong> procedure.<br />
Not everyone with hearing loss is a candidate for a <strong>Baha</strong>. <strong>Baha</strong> is contraindicated in<br />
patients with inadequate bone quality or quantity to provide stability and support for<br />
the implant, or in patients who will be unable to maintain and clean the skin around<br />
the abutment. In the U.S., use of the implanted fixture is also contraindicated in children<br />
under age 5 years.<br />
All surgical procedures include an element of risk, and it is impossible to guarantee success.<br />
The device may fail to osseointegrate for a number of reasons, including physiological<br />
and surgical issues as well as traumatic impact to the implant site. On rare occasions the<br />
skin around the abutment may become inflamed from a mild infection or the skin may<br />
grow back towards its original thickness. For complete information regarding the risks and<br />
benefits of a <strong>Baha</strong> procedure, please refer to the instructions for use for the <strong>Baha</strong> implant<br />
available at ww.<strong>Cochlear</strong>Americas.com/<strong>Baha</strong>indications<br />
www.<strong>Cochlear</strong>americas.com<br />
<strong>Cochlear</strong> americas<br />
13059 East Peakview avenue<br />
Centennial Co 80111<br />
uSa<br />
tel: 1 303 790 9010<br />
Fax: 1 303 792 9025<br />
<strong>Cochlear</strong> Canada inc<br />
2500-120 adelaide Street West<br />
toronto, on M5H 1t1<br />
Canada<br />
tel: 1 416 972 5082<br />
Fax: 1 416 972 5083<br />
<strong>Baha</strong> and <strong>Baha</strong> Divino are trademarks of <strong>Cochlear</strong> Bone anchored Solutions. <strong>Cochlear</strong> and the elliptical logo are<br />
trademarks of <strong>Cochlear</strong> Limited. the names of actual companies and products mentioned herein may be the<br />
trademarks of their respective owners. © <strong>Cochlear</strong> Bone anchored Solutions 2011.<br />
Bun070 iSS1 DEC11