Effect of screw diameter on orthodontic skeletal anchorage
Effect of screw diameter on orthodontic skeletal anchorage
Effect of screw diameter on orthodontic skeletal anchorage

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
ORIGINAL ARTICLE<br />
<str<strong>on</strong>g>Effect</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>screw</str<strong>on</strong>g> <str<strong>on</strong>g>diameter</str<strong>on</strong>g> <strong>on</strong> orthod<strong>on</strong>tic <strong>skeletal</strong><br />
<strong>anchorage</strong><br />
Chad Morarend, a Fang Qian, b Steve D. Marshall, c Karin A. Southard, d Nicole M. Grosland, e Teresa A. Morgan, f<br />
Michelle McManus, g and Thomas E. Southard h<br />
Dubuque and Iowa City, Iowa<br />
Introducti<strong>on</strong>: Many case reports have documented the successful use <str<strong>on</strong>g>of</str<strong>on</strong>g> titanium mini<str<strong>on</strong>g>screw</str<strong>on</strong>g>s for orthod<strong>on</strong>tic<br />
<strong>anchorage</strong>. However, the literature lacks a well-c<strong>on</strong>trolled study examining the effect <str<strong>on</strong>g>of</str<strong>on</strong>g> mini<str<strong>on</strong>g>screw</str<strong>on</strong>g> <str<strong>on</strong>g>diameter</str<strong>on</strong>g> <strong>on</strong><br />
<strong>anchorage</strong> force resistance. The purpose <str<strong>on</strong>g>of</str<strong>on</strong>g> this in-vitro study was to compare the force resistance <str<strong>on</strong>g>of</str<strong>on</strong>g> larger<str<strong>on</strong>g>diameter</str<strong>on</strong>g><br />
m<strong>on</strong>ocortical mini<str<strong>on</strong>g>screw</str<strong>on</strong>g>s to smaller-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> m<strong>on</strong>ocortical mini<str<strong>on</strong>g>screw</str<strong>on</strong>g>s; and to compare the force<br />
resistance <str<strong>on</strong>g>of</str<strong>on</strong>g> larger-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> m<strong>on</strong>ocortical mini<str<strong>on</strong>g>screw</str<strong>on</strong>g>s to smaller-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> bicortical mini<str<strong>on</strong>g>screw</str<strong>on</strong>g>s. Methods:<br />
Ninety-six titanium alloy <str<strong>on</strong>g>screw</str<strong>on</strong>g>s were placed into 24 hemisected maxillary and 24 hemisected mandibular<br />
specimens between the first and sec<strong>on</strong>d premolars. Specimens were randomly and evenly divided into<br />
2 groups. In the first group, 24 large-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> <str<strong>on</strong>g>screw</str<strong>on</strong>g>s (2.5 3 17 mm) and with 24 small-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> <str<strong>on</strong>g>screw</str<strong>on</strong>g>s<br />
(1.5 3 15 mm) were placed m<strong>on</strong>ocortically. In the sec<strong>on</strong>d group, 24 large-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> <str<strong>on</strong>g>screw</str<strong>on</strong>g>s (2.5 3 17 mm)<br />
were placed m<strong>on</strong>ocortically and 24 small-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> <str<strong>on</strong>g>screw</str<strong>on</strong>g>s (1.5 3 15 mm) were placed bicortically. All <str<strong>on</strong>g>screw</str<strong>on</strong>g>s<br />
were subjected to tangential force loading perpendicular to the mini<str<strong>on</strong>g>screw</str<strong>on</strong>g> with lateral displacement <str<strong>on</strong>g>of</str<strong>on</strong>g> 0.6 mm.<br />
Statistical analyses, including the paired-samples t test and the 2-samples t test, were used to quantify <str<strong>on</strong>g>screw</str<strong>on</strong>g><br />
force-deflecti<strong>on</strong> characteristics. One-way analysis <str<strong>on</strong>g>of</str<strong>on</strong>g> variance (ANOVA) with the post-hoc Tukey studentized<br />
range test was used to determine any significant differences, and the order <str<strong>on</strong>g>of</str<strong>on</strong>g> those differences, in force <strong>anchorage</strong><br />
values am<strong>on</strong>g the 3 <str<strong>on</strong>g>screw</str<strong>on</strong>g> types at maxillary and mandibular sites. Results: Mean mandibular and<br />
maxillary <strong>anchorage</strong> force values <str<strong>on</strong>g>of</str<strong>on</strong>g> the 2.5-mm m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s were significantly greater than those<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> the 1.5-mm m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s (P \0.01). No statistically significant differences in mean mandibular <strong>anchorage</strong><br />
force values were found between the 2.5-mm m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s and the 1.5-mm bicortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s.<br />
However, mean maxillary <strong>anchorage</strong> force values <str<strong>on</strong>g>of</str<strong>on</strong>g> the 1.5-mm bicortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s were significantly greater<br />
than those <str<strong>on</strong>g>of</str<strong>on</strong>g> the 2.5-mm m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s (P \0.01). Data analyzed with 1-way ANOVA with the posthoc<br />
Tukey studentized range tests indicated that the mean mandibular and maxillary force values <str<strong>on</strong>g>of</str<strong>on</strong>g> the<br />
2.5-mm m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s and the 1.5-mm bicortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s were significantly greater than those <str<strong>on</strong>g>of</str<strong>on</strong>g> the<br />
1.5-mm m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s (P\0.01). Based <strong>on</strong> the 2-samples t test, mean <strong>anchorage</strong> force values at mandibular<br />
sites were significantly greater than at maxillary sites for the 2.5-mm m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s and the 1.5mm<br />
m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s. There were no statistically significant differences in mean <strong>anchorage</strong> force values<br />
between maxillary and mandibular sites for the 1.5-mm bicortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s. C<strong>on</strong>clusi<strong>on</strong>s: In vitro, larger-<str<strong>on</strong>g>diameter</str<strong>on</strong>g><br />
(2.5 mm) m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s provide greater <strong>anchorage</strong> force resistance than do smaller-<str<strong>on</strong>g>diameter</str<strong>on</strong>g><br />
(1.5 mm) m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s in both the mandible and the maxilla. Smaller-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> (1.5 mm) bicortical<br />
<str<strong>on</strong>g>screw</str<strong>on</strong>g>s provide <strong>anchorage</strong> force resistance at least equal to larger-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> (2.5 mm) m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s.<br />
An alternative to placing a larger-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> mini<str<strong>on</strong>g>screw</str<strong>on</strong>g> for additi<strong>on</strong>al <strong>anchorage</strong> is a narrower bicortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>.<br />
(Am J Orthod Dent<str<strong>on</strong>g>of</str<strong>on</strong>g>acial Orthop 2009;136:224-9)<br />
Many case reports have documented the successful<br />
use <str<strong>on</strong>g>of</str<strong>on</strong>g> titanium mini<str<strong>on</strong>g>screw</str<strong>on</strong>g>s and variati<strong>on</strong>s<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> surgical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s used for rigid fixati<strong>on</strong><br />
to provide orthod<strong>on</strong>tic <strong>anchorage</strong> without patient<br />
a<br />
Private practice, Dubuque, Iowa.<br />
b<br />
Associate research scientist, Department <str<strong>on</strong>g>of</str<strong>on</strong>g> Preventive and Community<br />
Dentistry, College <str<strong>on</strong>g>of</str<strong>on</strong>g> Dentistry, University <str<strong>on</strong>g>of</str<strong>on</strong>g> Iowa, Iowa City.<br />
c<br />
Adjunct associate pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essor, Department <str<strong>on</strong>g>of</str<strong>on</strong>g> Orthod<strong>on</strong>tics, College <str<strong>on</strong>g>of</str<strong>on</strong>g> Dentistry,<br />
University <str<strong>on</strong>g>of</str<strong>on</strong>g> Iowa, Iowa City.<br />
d<br />
Pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essor, Department <str<strong>on</strong>g>of</str<strong>on</strong>g> Orthod<strong>on</strong>tics, College <str<strong>on</strong>g>of</str<strong>on</strong>g> Dentistry, University <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
Iowa, Iowa City.<br />
e<br />
Assistant pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essor, Department <str<strong>on</strong>g>of</str<strong>on</strong>g> Biomedical Engineering, College <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
Engineering, University <str<strong>on</strong>g>of</str<strong>on</strong>g> Iowa, Iowa City.<br />
f<br />
Assistant pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essor, Department <str<strong>on</strong>g>of</str<strong>on</strong>g> Oral and Maxill<str<strong>on</strong>g>of</str<strong>on</strong>g>acial Surgery, College <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
Dentistry, University <str<strong>on</strong>g>of</str<strong>on</strong>g> Iowa, Iowa City.<br />
g<br />
Postgraduate student, College <str<strong>on</strong>g>of</str<strong>on</strong>g> Dentistry, University <str<strong>on</strong>g>of</str<strong>on</strong>g> Iowa, Iowa City.<br />
224<br />
compliance. 1-6 Compared with traditi<strong>on</strong>al endosseous<br />
implants, mini<str<strong>on</strong>g>screw</str<strong>on</strong>g>s <str<strong>on</strong>g>of</str<strong>on</strong>g>fer distinct advantages as anchors:<br />
smaller size, flexibility in site placement, ease<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> placement, less patient trauma, and lower cost. 7,8<br />
h<br />
Pr<str<strong>on</strong>g>of</str<strong>on</strong>g>essor and head, Department <str<strong>on</strong>g>of</str<strong>on</strong>g> Orthod<strong>on</strong>tics, College <str<strong>on</strong>g>of</str<strong>on</strong>g> Dentistry, University<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> Iowa, Iowa City.<br />
Supported by the Dr. George Andreasen Memorial Fund.<br />
The authors report no commercial, proprietary, or financial interest in the products<br />
or companies described in this article.<br />
Reprint requests to: Thomas E. Southard, Department <str<strong>on</strong>g>of</str<strong>on</strong>g> Orthod<strong>on</strong>tics, College<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> Dentistry, University <str<strong>on</strong>g>of</str<strong>on</strong>g> Iowa, Iowa City, IA 52242; e-mail, tom-southard@<br />
uiowa.edu.<br />
Submitted, May 2007; revised and accepted, July 2007.<br />
0889-5406/$36.00<br />
Copyright Ó 2009 by the American Associati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> Orthod<strong>on</strong>tists.<br />
doi:10.1016/j.ajodo.2007.07.031
American Journal <str<strong>on</strong>g>of</str<strong>on</strong>g> Orthod<strong>on</strong>tics and Dent<str<strong>on</strong>g>of</str<strong>on</strong>g>acial Orthopedics Morarend et al 225<br />
Volume 136, Number 2<br />
Additi<strong>on</strong>ally, because the primary stability <str<strong>on</strong>g>of</str<strong>on</strong>g> mini<str<strong>on</strong>g>screw</str<strong>on</strong>g>s<br />
is believed to result from mechanical interlock,<br />
a waiting period for osseointegrati<strong>on</strong> before orthod<strong>on</strong>tic<br />
loading is unnecessary, as is a sec<strong>on</strong>d surgical procedure<br />
(trephinati<strong>on</strong>) for removal. 1,8,9 On the other hand, because<br />
mini<str<strong>on</strong>g>screw</str<strong>on</strong>g>s are not osseointegrated, their <strong>anchorage</strong><br />
potential is most likely influenced by the quality<br />
and quantity <str<strong>on</strong>g>of</str<strong>on</strong>g> b<strong>on</strong>e into which they are placed. 10<br />
Case reports have documented problems associated<br />
with mini<str<strong>on</strong>g>screw</str<strong>on</strong>g> <strong>anchorage</strong>, including peri<str<strong>on</strong>g>screw</str<strong>on</strong>g> inflammati<strong>on</strong><br />
and <str<strong>on</strong>g>screw</str<strong>on</strong>g> mobility. 11-13 In a prospective study<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> risk factors associated with mini<str<strong>on</strong>g>screw</str<strong>on</strong>g> failures,<br />
Cheng et al 13 reported that length had no significant<br />
effect <strong>on</strong> <str<strong>on</strong>g>screw</str<strong>on</strong>g> survival and that loads <str<strong>on</strong>g>of</str<strong>on</strong>g> 100 to 200 g<br />
could be sustained with no significant differences between<br />
successful and failed <str<strong>on</strong>g>screw</str<strong>on</strong>g>s. Although other<br />
researchers identified no major differences in the survival<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> mini<str<strong>on</strong>g>screw</str<strong>on</strong>g>s placed in keratinized or n<strong>on</strong>keratinized<br />
mucosa, 14,15 Cheng et al 13 advised placing them<br />
in keratinized mucosa and using cauti<strong>on</strong> when working<br />
in dense b<strong>on</strong>e regi<strong>on</strong>s such as the posterior mandible to<br />
avoid b<strong>on</strong>e overheating.<br />
It was suggested that the type <str<strong>on</strong>g>of</str<strong>on</strong>g> force system used<br />
can lead to <str<strong>on</strong>g>screw</str<strong>on</strong>g> failure. 1 Huja et al 10 cauti<strong>on</strong>ed that<br />
torsi<strong>on</strong>al loading <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>screw</str<strong>on</strong>g>s might deb<strong>on</strong>d any mechanical<br />
or chemical integrati<strong>on</strong> between the <str<strong>on</strong>g>screw</str<strong>on</strong>g> and b<strong>on</strong>e<br />
interface. Using maxillae and mandibular cadaver specimens,<br />
Brettin et al 16 tested the hypothesis that bicortical<br />
mini<str<strong>on</strong>g>screw</str<strong>on</strong>g> placement (across the entire width <str<strong>on</strong>g>of</str<strong>on</strong>g> the<br />
alveolus) could provide a force system with superior<br />
force resistance and stability (<strong>anchorage</strong>) compared<br />
with m<strong>on</strong>ocortical placement. Deflecti<strong>on</strong> force values<br />
were significantly greater for bicortical than for m<strong>on</strong>ocortical<br />
<str<strong>on</strong>g>screw</str<strong>on</strong>g>s. The authors c<strong>on</strong>cluded that bicortical<br />
mini<str<strong>on</strong>g>screw</str<strong>on</strong>g> placement provides superior <strong>anchorage</strong> resistance,<br />
reduced cortical b<strong>on</strong>e stress, and superior<br />
stability than m<strong>on</strong>ocortical placement.<br />
In a retrospective study, Miyawaki et al 17 correlated<br />
several variables with the success <str<strong>on</strong>g>of</str<strong>on</strong>g> 134 m<strong>on</strong>ocortical<br />
<str<strong>on</strong>g>screw</str<strong>on</strong>g>s. Success rates <str<strong>on</strong>g>of</str<strong>on</strong>g> 0.0%, 83.9%, and 85% were<br />
found with <str<strong>on</strong>g>screw</str<strong>on</strong>g> <str<strong>on</strong>g>diameter</str<strong>on</strong>g>s <str<strong>on</strong>g>of</str<strong>on</strong>g> 1.0, 1.5, and 2.3 mm,<br />
respectively. A high mandibular plane angle was also<br />
found to be associated with a significantly lower success<br />
rate, but no significant correlati<strong>on</strong> was found between<br />
success rate and <str<strong>on</strong>g>screw</str<strong>on</strong>g> length, type <str<strong>on</strong>g>of</str<strong>on</strong>g> placement surgery,<br />
immediate loading, age, sex, crowding, anteroposterior<br />
jaw base relati<strong>on</strong>ship, c<strong>on</strong>trolled period<strong>on</strong>titis, or<br />
temporomandibular joint disorder symptoms.<br />
The wide range <str<strong>on</strong>g>of</str<strong>on</strong>g> reported mini<str<strong>on</strong>g>screw</str<strong>on</strong>g> success rates<br />
and the absence <str<strong>on</strong>g>of</str<strong>on</strong>g> accepted clinical protocols suggest<br />
the need for further research <str<strong>on</strong>g>of</str<strong>on</strong>g> these temporary <strong>anchorage</strong><br />
devices. The literature lacks a well-c<strong>on</strong>trolled study<br />
examining the effect <str<strong>on</strong>g>of</str<strong>on</strong>g> mini<str<strong>on</strong>g>screw</str<strong>on</strong>g> <str<strong>on</strong>g>diameter</str<strong>on</strong>g> <strong>on</strong> anchor-<br />
age force resistance. The objective <str<strong>on</strong>g>of</str<strong>on</strong>g> this in-vitro study<br />
was to examine this effect. Specifically, the force resistance<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> a larger-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> m<strong>on</strong>ocortical mini<str<strong>on</strong>g>screw</str<strong>on</strong>g> was<br />
compared with that <str<strong>on</strong>g>of</str<strong>on</strong>g> a smaller-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> m<strong>on</strong>ocortical<br />
mini<str<strong>on</strong>g>screw</str<strong>on</strong>g>, and the force resistance <str<strong>on</strong>g>of</str<strong>on</strong>g> a larger-<str<strong>on</strong>g>diameter</str<strong>on</strong>g><br />
m<strong>on</strong>ocortical mini<str<strong>on</strong>g>screw</str<strong>on</strong>g> was compared with that <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
a smaller-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> bicortical mini<str<strong>on</strong>g>screw</str<strong>on</strong>g>.<br />
MATERIAL AND METHODS<br />
The maxillae and mandibles <str<strong>on</strong>g>of</str<strong>on</strong>g> human cadavers were<br />
obtained from the Department <str<strong>on</strong>g>of</str<strong>on</strong>g> Anatomy and Cell Biology<br />
Deeded Body Program at the University <str<strong>on</strong>g>of</str<strong>on</strong>g> Iowa.<br />
Fully dentate and partially dentate specimens were c<strong>on</strong>sidered<br />
acceptable. Fully edentulous or partially dentate<br />
specimens with visible, severely atrophic alveolar ridges<br />
were excluded. Maxillary specimens were dissected superior<br />
to the maxillary sinus to avoid damage to the maxillary<br />
alveolar b<strong>on</strong>e and tooth roots and extended distally<br />
to the maxillary tuberosity. Mandibular specimens were<br />
dissected approximately halfway up the ascending ramus.<br />
All maxillae and mandibles were then hemisected,<br />
s<str<strong>on</strong>g>of</str<strong>on</strong>g>t tissue was carefully removed, and they were stored<br />
in 10% buffered formalin soluti<strong>on</strong>.<br />
Periapical radiographs <str<strong>on</strong>g>of</str<strong>on</strong>g> each specimen were made<br />
to verify adequate b<strong>on</strong>e and proper root divergence between<br />
adjacent teeth for placement <str<strong>on</strong>g>of</str<strong>on</strong>g> the mini<str<strong>on</strong>g>screw</str<strong>on</strong>g>s.<br />
The site for placement was between the first and sec<strong>on</strong>d<br />
premolars in both jaws. Twenty-four maxillae from different<br />
cadavers and 24 mandibles from different cadavers<br />
were used. If either the first or sec<strong>on</strong>d premolar<br />
was missing, the adjacent first or sec<strong>on</strong>d premolar was<br />
used as a reference for <str<strong>on</strong>g>screw</str<strong>on</strong>g> locati<strong>on</strong> based <strong>on</strong> average<br />
tooth size. After radiographic examinati<strong>on</strong>, 12 right and<br />
12 left hemi-maxillae from different cadavers, and<br />
12 right and 12 left hemi-mandibles from different<br />
cadavers, were deemed acceptable.<br />
In the first experiment (larger-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> vs smaller<str<strong>on</strong>g>diameter</str<strong>on</strong>g><br />
m<strong>on</strong>ocortical <strong>anchorage</strong>), 48 commercially<br />
available titanium <str<strong>on</strong>g>screw</str<strong>on</strong>g>s (KLS Martin, Jacks<strong>on</strong>ville,<br />
Fla) were placed in 12 hemisected maxillae and 12 hemisected<br />
mandibles. Twenty-four large-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> <str<strong>on</strong>g>screw</str<strong>on</strong>g>s<br />
(2.5 3 17 mm) (#25-674-17-1, KLS Martin) and 24<br />
small-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> <str<strong>on</strong>g>screw</str<strong>on</strong>g>s (1.5 3 15 mm) (#25-675-15, KLS<br />
Martin)wereplacedm<strong>on</strong>ocortically.Inthesec<strong>on</strong>dexperiment<br />
(larger-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> m<strong>on</strong>ocortical vs smaller-<str<strong>on</strong>g>diameter</str<strong>on</strong>g><br />
bicortical <strong>anchorage</strong>), 48 <str<strong>on</strong>g>screw</str<strong>on</strong>g>s were likewise placed in<br />
12 hemisected maxillae and 12 hemisected mandibles.<br />
Twenty-four large-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> <str<strong>on</strong>g>screw</str<strong>on</strong>g>s (2.5 3 17 mm) were<br />
placed m<strong>on</strong>ocortically, and 24 small-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> <str<strong>on</strong>g>screw</str<strong>on</strong>g>s<br />
(1.5315mm)wereplacedbicortically.<br />
For each b<strong>on</strong>e specimen, 2 <str<strong>on</strong>g>screw</str<strong>on</strong>g>s were placed<br />
between the first and sec<strong>on</strong>d premolars with 1 more
226 Morarend et al American Journal <str<strong>on</strong>g>of</str<strong>on</strong>g> Orthod<strong>on</strong>tics and Dent<str<strong>on</strong>g>of</str<strong>on</strong>g>acial Orthopedics<br />
August 2009<br />
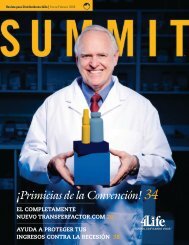
Fig 1. Mini<str<strong>on</strong>g>screw</str<strong>on</strong>g> placement distances from crestal<br />
b<strong>on</strong>e: 1.5-mm <str<strong>on</strong>g>diameter</str<strong>on</strong>g> <str<strong>on</strong>g>screw</str<strong>on</strong>g> in cor<strong>on</strong>al positi<strong>on</strong> and<br />
2.5-mm <str<strong>on</strong>g>diameter</str<strong>on</strong>g> <str<strong>on</strong>g>screw</str<strong>on</strong>g> in apical positi<strong>on</strong>.<br />
cor<strong>on</strong>ally positi<strong>on</strong>ed and the other more apically positi<strong>on</strong>ed<br />
(Fig 1). The cor<strong>on</strong>ally positi<strong>on</strong>ed <str<strong>on</strong>g>screw</str<strong>on</strong>g> was<br />
placed 5 mm apical to the maximum height <str<strong>on</strong>g>of</str<strong>on</strong>g> the interproximal<br />
crestal b<strong>on</strong>e. The apically positi<strong>on</strong>ed <str<strong>on</strong>g>screw</str<strong>on</strong>g><br />
was placed 4.5 mm apical to the cor<strong>on</strong>ally positi<strong>on</strong>ed<br />
<str<strong>on</strong>g>screw</str<strong>on</strong>g>. These distances were selected to ensure that all<br />
<str<strong>on</strong>g>screw</str<strong>on</strong>g>s would have adequate b<strong>on</strong>e and proper root divergence<br />
without root c<strong>on</strong>tact, would not be placed in the<br />
mental foramen or the maxillary sinus areas, and would<br />
have adequate separati<strong>on</strong>. Based <strong>on</strong> average b<strong>on</strong>e thickness<br />
values, the m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s were placed to<br />
a depth <str<strong>on</strong>g>of</str<strong>on</strong>g> 4 mm to ensure complete penetrati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> the<br />
buccal plate without engaging the lingual cortical<br />
plate. 16 Bicortical placement was verified by visual observati<strong>on</strong><br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> the <str<strong>on</strong>g>screw</str<strong>on</strong>g> as it began to protrude through the<br />
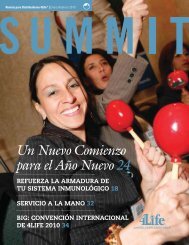
external surface <str<strong>on</strong>g>of</str<strong>on</strong>g> the lingual cortical b<strong>on</strong>e. Figure 2<br />
shows m<strong>on</strong>ocortical and bicortical <str<strong>on</strong>g>screw</str<strong>on</strong>g> placements<br />
and force applicati<strong>on</strong>s from an orthog<strong>on</strong>al view.<br />
For each experiment, b<strong>on</strong>e specimen assignments<br />
were made to ensure an even and random distributi<strong>on</strong><br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>screw</str<strong>on</strong>g> <str<strong>on</strong>g>diameter</str<strong>on</strong>g>s between maxillary and mandibular<br />
b<strong>on</strong>e specimens, right and left b<strong>on</strong>e specimens, and cor<strong>on</strong>al<br />
and apical b<strong>on</strong>e sites. All <str<strong>on</strong>g>screw</str<strong>on</strong>g>s were placed by 1<br />
operator (C.M.) with a hand driver (blade #25-483-97,<br />
handle #25-402-99, KLS Martin) after pilot hole drilling<br />
with the manufacturer’s recommended n<strong>on</strong>tapered,<br />
1.1-mm <str<strong>on</strong>g>diameter</str<strong>on</strong>g> twist drill for the 1.5-mm <str<strong>on</strong>g>screw</str<strong>on</strong>g>s (#25-<br />
452-15, KLS Martin) and 1.9-mm <str<strong>on</strong>g>diameter</str<strong>on</strong>g> twist drill<br />
for the 2.5-mm <str<strong>on</strong>g>screw</str<strong>on</strong>g>s (#25-460-19, KLS Martin). A<br />
n<strong>on</strong>tapered drill was used to ensure no differences in<br />
hole sizes for the bicortical samples, since all <str<strong>on</strong>g>screw</str<strong>on</strong>g>s<br />
had a uniform <str<strong>on</strong>g>diameter</str<strong>on</strong>g> throughout. All <str<strong>on</strong>g>screw</str<strong>on</strong>g>s were<br />
placed perpendicular to the buccal b<strong>on</strong>e surface and parallel<br />
to the occlusal plane.<br />
Fig 2. M<strong>on</strong>ocortical and bicortical mini<str<strong>on</strong>g>screw</str<strong>on</strong>g> placements,<br />
orthog<strong>on</strong>al view.<br />
After <str<strong>on</strong>g>screw</str<strong>on</strong>g> placement, periapical radiographs were<br />
taken <str<strong>on</strong>g>of</str<strong>on</strong>g> all specimens to ensure that the <str<strong>on</strong>g>screw</str<strong>on</strong>g>s had not<br />
violated the mental foramen, the maxillary sinus, and<br />
the roots <str<strong>on</strong>g>of</str<strong>on</strong>g> any teeth. After verificati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> satisfactory<br />
<str<strong>on</strong>g>screw</str<strong>on</strong>g> placement, the most distal porti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> each b<strong>on</strong>y<br />
specimen was embedded in buff laboratory st<strong>on</strong>e to<br />
a depth <str<strong>on</strong>g>of</str<strong>on</strong>g> 1.0 in and allowed to harden for 24 hours<br />
in preparati<strong>on</strong> for force applicati<strong>on</strong>.<br />
To mimic orthod<strong>on</strong>tic force, each mini<str<strong>on</strong>g>screw</str<strong>on</strong>g> was subjected<br />
to a tangential force oriented perpendicular to the<br />
mini<str<strong>on</strong>g>screw</str<strong>on</strong>g> (Fig 2).Acustomizedx-y-z tablewith a mounting<br />
device (Brettin et al 16 ) was fabricated to rigidly fixate<br />
andorienteachspecimenembeddedinast<strong>on</strong>eblock<br />
during testing. Furthermore, a customized grip was designed<br />
and machined from stainless steel to fit between<br />
the threads <str<strong>on</strong>g>of</str<strong>on</strong>g> each mini<str<strong>on</strong>g>screw</str<strong>on</strong>g> and apply a tangential<br />
load at a distance <str<strong>on</strong>g>of</str<strong>on</strong>g> 3 mm from the <str<strong>on</strong>g>screw</str<strong>on</strong>g>-b<strong>on</strong>e interface.<br />
This distance represented a reas<strong>on</strong>able space that would<br />
be typically occupied by s<str<strong>on</strong>g>of</str<strong>on</strong>g>t tissue in vivo.<br />
Each mini<str<strong>on</strong>g>screw</str<strong>on</strong>g> was subjected to a tangential force<br />
load perpendicular to the <str<strong>on</strong>g>screw</str<strong>on</strong>g> but parallel to the occlusal<br />
plane by using an Instr<strong>on</strong> diametral materials testing<br />
machine (model 1445, Zwick GmbH, Ulm, Germany).<br />
The crosshead speed was set at 0.05 mm per sec<strong>on</strong>d. 10,16<br />
During loading, displacement <str<strong>on</strong>g>of</str<strong>on</strong>g> each <str<strong>on</strong>g>screw</str<strong>on</strong>g> was measured<br />
up to 0.6 mm, which, from pilot studies, represented<br />
adequate displacement without slippage at the<br />
<str<strong>on</strong>g>screw</str<strong>on</strong>g>-thread/grip interface.<br />
Each <str<strong>on</strong>g>screw</str<strong>on</strong>g> was removed, and the b<strong>on</strong>y specimens<br />
were secti<strong>on</strong>ed at the mesial and distal aspects <str<strong>on</strong>g>of</str<strong>on</strong>g> the<br />
mini<str<strong>on</strong>g>screw</str<strong>on</strong>g> placement site to allow b<strong>on</strong>e thickness
American Journal <str<strong>on</strong>g>of</str<strong>on</strong>g> Orthod<strong>on</strong>tics and Dent<str<strong>on</strong>g>of</str<strong>on</strong>g>acial Orthopedics Morarend et al 227<br />
Volume 136, Number 2<br />
Fig 3. Mean <strong>anchorage</strong> force values (in newt<strong>on</strong>s) vs<br />
<str<strong>on</strong>g>screw</str<strong>on</strong>g> deflecti<strong>on</strong> for 2.5-mm m<strong>on</strong>ocortical (m<strong>on</strong>o)<br />
<str<strong>on</strong>g>screw</str<strong>on</strong>g>s and 1.5-mm m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s in the mandible<br />
(Md) and the maxilla (Mx).<br />
visualizati<strong>on</strong> and measurement. Buccal cortical plate,<br />
lingual cortical plate, and total alveolar b<strong>on</strong>e width<br />
were measured by 1 observer (C.M.) with a fine-tip digital<br />
caliper. Each measurement was made twice at each<br />
<str<strong>on</strong>g>screw</str<strong>on</strong>g> placement site, and the average <str<strong>on</strong>g>of</str<strong>on</strong>g> the measurements<br />
was recorded.<br />
Statistical analyis<br />
A paired-samples t test was used to determine<br />
whether there were significant differences in force <strong>anchorage</strong><br />
at each deflecti<strong>on</strong> value for both mandibular<br />
and maxillary sites: between the 2 <str<strong>on</strong>g>diameter</str<strong>on</strong>g>s <str<strong>on</strong>g>of</str<strong>on</strong>g> m<strong>on</strong>ocortical<br />
<str<strong>on</strong>g>screw</str<strong>on</strong>g>s (2.5 and 1.5 mm) and between the<br />
larger-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g> (2.5 mm) and the<br />
smaller-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> bicortical <str<strong>on</strong>g>screw</str<strong>on</strong>g> (1.5 mm). A 2-samples<br />
t test was used to determine whether there were significant<br />
differences in force <strong>anchorage</strong> values between<br />
maxillary and mandibular, right and left, and apical<br />
and cor<strong>on</strong>al sites for the 2.5-mm m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s,<br />
the 1.5-mm m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s, and the 1.5-mm<br />
bicortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s. One-way analysis <str<strong>on</strong>g>of</str<strong>on</strong>g> variance (AN-<br />
OVA) with the post-hoc Tukey studentized range test<br />
was used to determine whether there were significant<br />
differences and the order <str<strong>on</strong>g>of</str<strong>on</strong>g> those differences in force<br />
<strong>anchorage</strong> values am<strong>on</strong>g the 3 <str<strong>on</strong>g>screw</str<strong>on</strong>g> types at the maxillary<br />
and mandibular sites. Means and standard deviati<strong>on</strong>s<br />
were calculated for b<strong>on</strong>e thicknesses. All data<br />
analysis was c<strong>on</strong>ducted by using SAS s<str<strong>on</strong>g>of</str<strong>on</strong>g>tware (versi<strong>on</strong><br />
9.1, SAS, Cary, NC) at either the 0.05 or 0.01 level <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
statistical significance.<br />
RESULTS<br />
Data analysis showed (Figs 3 and 4) that the mean<br />
mandibular <strong>anchorage</strong> force values <str<strong>on</strong>g>of</str<strong>on</strong>g> the 2.5-mm<br />
m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s were significantly greater than<br />
Fig 4. Mean <strong>anchorage</strong> force values vs <str<strong>on</strong>g>screw</str<strong>on</strong>g> deflecti<strong>on</strong><br />
for 2.5-mm m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s and 1.5-mm bicortical<br />
(bi) <str<strong>on</strong>g>screw</str<strong>on</strong>g>s.<br />
those <str<strong>on</strong>g>of</str<strong>on</strong>g> the 1.5-mm m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s when the deflecti<strong>on</strong><br />
increased from 0.04 to 0.6 mm (P \0.01).<br />
Moreover, the mean maxillary <strong>anchorage</strong> force values<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> the 2.5-mm m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s were significantly<br />
greater than those for the 1.5-mm m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s<br />
when the deflecti<strong>on</strong> increased from 0.14 to 0.6 mm<br />
(P \0.01).<br />
No statistically significant differences in mean mandibular<br />
<strong>anchorage</strong> force values were found between the<br />
2.5 mm m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s and the 1.5-mm bicortical<br />
<str<strong>on</strong>g>screw</str<strong>on</strong>g>s. However, the mean maxillary <strong>anchorage</strong> force<br />
values <str<strong>on</strong>g>of</str<strong>on</strong>g> the 1.5 mm bicortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s were significantly<br />
greater than those <str<strong>on</strong>g>of</str<strong>on</strong>g> the 2.5-mm m<strong>on</strong>ocortical<br />
<str<strong>on</strong>g>screw</str<strong>on</strong>g>s when the deflecti<strong>on</strong> increased from 0.11 to<br />
0.6 mm (P \0.01).<br />
Data analyzed with 1-way ANOVA with the posthoc<br />
Tukey studentized range tests indicated that the<br />
mean force values <str<strong>on</strong>g>of</str<strong>on</strong>g> the 2.5-mm m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s<br />
and the 1.5-mm bicortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s were significantly<br />
greater than those <str<strong>on</strong>g>of</str<strong>on</strong>g> the 1.5-mm m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s<br />
when mandibular deflecti<strong>on</strong> increased from 0.04 to<br />
0.6 mm, or maxillary deflecti<strong>on</strong> increased from 0.07<br />
to 0.60 mm (P \0.01). There were no significant<br />
differences between the 2.5-mm m<strong>on</strong>ocortical and the<br />
1.5-mm bicortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s.<br />
Mean <strong>anchorage</strong> force values at mandibular sites<br />
were significantly greater than at maxillary sites for<br />
the 2.5-mm m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s when the deflecti<strong>on</strong> increased<br />
from 0.11 to 0.60 mm (P\0.05). Mean <strong>anchorage</strong><br />
force values at mandibular sites were significantly<br />
greater than at maxillary sites for the 1.5-mm m<strong>on</strong>ocortical<br />
<str<strong>on</strong>g>screw</str<strong>on</strong>g>s when the deflecti<strong>on</strong> increased from 0.24 to<br />
0.60 mm (P \0.05). There were no statistically significant<br />
differences in mean <strong>anchorage</strong> force values between<br />
maxillary and mandibular sites for the 1.5-mm<br />
bicortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s. There were no significant differences<br />
in mean <strong>anchorage</strong> force values between the right and
228 Morarend et al American Journal <str<strong>on</strong>g>of</str<strong>on</strong>g> Orthod<strong>on</strong>tics and Dent<str<strong>on</strong>g>of</str<strong>on</strong>g>acial Orthopedics<br />
August 2009<br />
left sides for any <str<strong>on</strong>g>screw</str<strong>on</strong>g> type. Moreover, there were no<br />
significant differences in mean <strong>anchorage</strong> force values<br />
between cor<strong>on</strong>al and apical positi<strong>on</strong>s for any <str<strong>on</strong>g>screw</str<strong>on</strong>g><br />
type. B<strong>on</strong>e thickness means (SD) for maxillary labial,<br />
maxillary lingual, mandibular labial, and mandibular<br />
lingual cortical b<strong>on</strong>e were 2.11 (0.39), 2.01 (0.70),<br />
2.15 (0.62), and 2.97 (0.69) mm, respectively.<br />
DISCUSSION<br />
Two principal findings resulted from this in-vitro<br />
study. The first was that larger-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> m<strong>on</strong>ocortical<br />
<str<strong>on</strong>g>screw</str<strong>on</strong>g>s provide increased <strong>anchorage</strong> force resistance<br />
compared with smaller-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s.<br />
As illustrated in Figure 3, the mean <strong>anchorage</strong> force<br />
values <str<strong>on</strong>g>of</str<strong>on</strong>g> the 2.5-mm m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s exceeded<br />
those <str<strong>on</strong>g>of</str<strong>on</strong>g> the 1.5-mm m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s in both the mandible<br />
and the maxilla (P\0.01). The sec<strong>on</strong>d finding was<br />
that smaller-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> bicortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s can provide <strong>anchorage</strong><br />
resistance equal to, or even greater than, larger<str<strong>on</strong>g>diameter</str<strong>on</strong>g><br />
m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s. As shown in Figure 4,<br />
the mean <strong>anchorage</strong> force values <str<strong>on</strong>g>of</str<strong>on</strong>g> the 1.5-mm bicortical<br />
<str<strong>on</strong>g>screw</str<strong>on</strong>g>s were comparable with the values for the 2.5-mm<br />
m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s in the mandible but exceeded the<br />
values for the 2.5-mm m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s (P \0.01)<br />
in the maxilla.<br />
Additi<strong>on</strong>ally, as shown in these figures, mandibular<br />
b<strong>on</strong>e sites <str<strong>on</strong>g>of</str<strong>on</strong>g>fered significantly greater mean force resistance<br />
than did maxillary b<strong>on</strong>e sites (P \0.05) for both<br />
1.5- and 2.5-mm m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s. This finding<br />
agrees with that <str<strong>on</strong>g>of</str<strong>on</strong>g> Brettin et al 16 but is surprising because<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> the similar mandibular and maxillary labial<br />
cortical thicknesses measured in this sample. However,<br />
this similarity in thickness could help to explain the<br />
n<strong>on</strong>significant difference between maxillary and mandibular<br />
b<strong>on</strong>e sites for the 1.5-mm bicortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s.<br />
The n<strong>on</strong>significance between the right and left sites<br />
was expected. However, the n<strong>on</strong>significance between<br />
cor<strong>on</strong>al and apical sites, as also reported by Brettin et<br />
al, 16 is <str<strong>on</strong>g>of</str<strong>on</strong>g> interest and might be valuable to practicing orthod<strong>on</strong>tists.<br />
That is, since vertical placement, within the<br />
limits here, does not impact mean <strong>anchorage</strong> force resistance,<br />
placement <str<strong>on</strong>g>of</str<strong>on</strong>g> either a m<strong>on</strong>ocortical or a bicortical<br />
<str<strong>on</strong>g>screw</str<strong>on</strong>g> in a more cor<strong>on</strong>al positi<strong>on</strong> (in attached gingiva)<br />
makes sense to limit the possibility <str<strong>on</strong>g>of</str<strong>on</strong>g> peri-implant inflammati<strong>on</strong>.<br />
8,17 In additi<strong>on</strong> to providing an envir<strong>on</strong>ment<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> reduced inflammati<strong>on</strong>, the cor<strong>on</strong>al placement <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
<str<strong>on</strong>g>screw</str<strong>on</strong>g>s might be biomechanically advantageous because<br />
they are closer to the center <str<strong>on</strong>g>of</str<strong>on</strong>g> resistance <str<strong>on</strong>g>of</str<strong>on</strong>g> the teeth.<br />
Our finding that a 2.5-mm m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g> provides<br />
superior <strong>anchorage</strong> resistance compared with<br />
a 1.5-mm m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g> c<strong>on</strong>trasts with the findings<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> Miyawaki et al, 17 who reported no difference<br />
in the 1-year success rates <str<strong>on</strong>g>of</str<strong>on</strong>g> 2.3 and 1.5 mm <str<strong>on</strong>g>screw</str<strong>on</strong>g>s<br />
(85% and 84% successes, respectively). But they also<br />
reported a success rate <str<strong>on</strong>g>of</str<strong>on</strong>g> 0.0% for the 1.0-mm <str<strong>on</strong>g>diameter</str<strong>on</strong>g><br />
<str<strong>on</strong>g>screw</str<strong>on</strong>g>s. Thus, <str<strong>on</strong>g>diameter</str<strong>on</strong>g> does appear to play a role clinically,<br />
but the effect might be less pr<strong>on</strong>ounced at lower<br />
loading with larger-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> <str<strong>on</strong>g>screw</str<strong>on</strong>g>s.<br />
The biologic changes <strong>on</strong> osseous loading could not<br />
be examined in this in-vitro study. However, unlike<br />
traditi<strong>on</strong>al endosseous implants, which need a waiting<br />
period for b<strong>on</strong>e healing and osseointegrati<strong>on</strong>, the primary<br />
stability <str<strong>on</strong>g>of</str<strong>on</strong>g> mini<str<strong>on</strong>g>screw</str<strong>on</strong>g>s is believed to result from<br />
mechanical retenti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> the <str<strong>on</strong>g>screw</str<strong>on</strong>g> in the b<strong>on</strong>e. 1,9 In-vitro<br />
studies <str<strong>on</strong>g>of</str<strong>on</strong>g> mini<str<strong>on</strong>g>screw</str<strong>on</strong>g>s should, therefore, more<br />
closely replicate their immediate loading resp<strong>on</strong>se in<br />
situ after placement.<br />
Recently, Huja et al 10 reported the pull-out strengths<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s placed in the maxillae and mandibles<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> dogs. Pull-out forces ranged from 134 to 388<br />
N; these forces are somewhat greater than, but similar<br />
to, the force levels we reported here. Although these<br />
force levels are greater than those normally used to<br />
move teeth, well-c<strong>on</strong>trolled in-vitro studies such as<br />
these provide valuable insights into <strong>anchorage</strong>. Furthermore,<br />
greater forces are <str<strong>on</strong>g>of</str<strong>on</strong>g>ten used by orthod<strong>on</strong>tists to<br />
treat patients orthopedically. For instance, after placement<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> miniplates <strong>on</strong> the lateral nasal wall for <strong>anchorage</strong>,<br />
Kircelli et al 18 applied facemask protracti<strong>on</strong> to an<br />
11-year-old girl with severe maxillary hypoplasia. The<br />
forces applied to the plates were 150 to 350 g.<br />
Clinically, the advantage <str<strong>on</strong>g>of</str<strong>on</strong>g> a larger (m<strong>on</strong>ocortical)<br />
<str<strong>on</strong>g>screw</str<strong>on</strong>g> is its ability to distribute applied forces over<br />
greater areas <str<strong>on</strong>g>of</str<strong>on</strong>g> b<strong>on</strong>e with less b<strong>on</strong>e stress. For this reas<strong>on</strong>,<br />
when smaller m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s loosen in thin<br />
cortical b<strong>on</strong>e and cannot be retightened, they are typically<br />
replaced with larger <str<strong>on</strong>g>screw</str<strong>on</strong>g>s. The drawback <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
a larger <str<strong>on</strong>g>screw</str<strong>on</strong>g> is the surrounding anatomic limitati<strong>on</strong>s.<br />
The results <str<strong>on</strong>g>of</str<strong>on</strong>g> this study indicate that another alternative<br />
is a narrower bicortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>. A bicortical small-<str<strong>on</strong>g>diameter</str<strong>on</strong>g><br />
<str<strong>on</strong>g>screw</str<strong>on</strong>g> is particularly useful when there is insufficient<br />
room interproximally to place a larger-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> m<strong>on</strong>ocortical<br />
<str<strong>on</strong>g>screw</str<strong>on</strong>g>. Especially in patients with thin maxillary<br />
cortical b<strong>on</strong>e, a bicortical <str<strong>on</strong>g>screw</str<strong>on</strong>g> might be the mini<str<strong>on</strong>g>screw</str<strong>on</strong>g><br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> choice. The advantage is the same, or better, <strong>anchorage</strong><br />
resistance as a larger-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> <str<strong>on</strong>g>screw</str<strong>on</strong>g>. The disadvantage<br />
is that the pilot hole must be drilled through both<br />
cortices; this might be difficult in the posterior areas,<br />
where cheek retracti<strong>on</strong> is a limitati<strong>on</strong>.<br />
CONCLUSIONS<br />
1. In vitro, larger-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> (2.5 mm) m<strong>on</strong>ocortical<br />
<str<strong>on</strong>g>screw</str<strong>on</strong>g>s provide increased <strong>anchorage</strong> force resistance<br />
compared with smaller-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> (1.5 mm)
American Journal <str<strong>on</strong>g>of</str<strong>on</strong>g> Orthod<strong>on</strong>tics and Dent<str<strong>on</strong>g>of</str<strong>on</strong>g>acial Orthopedics Morarend et al 229<br />
Volume 136, Number 2<br />
m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s in both the mandible and the<br />
maxilla.<br />
2. Smaller-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> (1.5 mm) bicortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s provide<br />
<strong>anchorage</strong> force resistance at least equal to<br />
larger-<str<strong>on</strong>g>diameter</str<strong>on</strong>g> (2.5 mm) m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s.<br />
3. Mini<str<strong>on</strong>g>screw</str<strong>on</strong>g> <strong>anchorage</strong> force resistance is independent<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> the side <str<strong>on</strong>g>of</str<strong>on</strong>g> either the maxilla or the mandible.<br />
Force resistance is independent <str<strong>on</strong>g>of</str<strong>on</strong>g> apical or<br />
cor<strong>on</strong>al site placement, within the limits <str<strong>on</strong>g>of</str<strong>on</strong>g> this<br />
study, for either the maxilla or the mandible.<br />
REFERENCES<br />
1. Costa A, Raffaini M, Melsen B. Mini<str<strong>on</strong>g>screw</str<strong>on</strong>g>s as orthod<strong>on</strong>tic <strong>anchorage</strong>:<br />
a preliminary report. Int J Adult Orthod Orthognath<br />
Surg 1998;13:201-9.<br />
2. Gelgor IE, Buyukyilmaz T, Karaman AI, Dolanmaz D, Kalayci A.<br />
Intraosseous <str<strong>on</strong>g>screw</str<strong>on</strong>g>-supported upper molar distalizati<strong>on</strong>. Angle<br />
Orthod 2004;74:838-50.<br />
3. Kuroda S, Katayama A, Takano-Yamamoto T. Severe anterior<br />
open-bite case treated using titanium <str<strong>on</strong>g>screw</str<strong>on</strong>g> <strong>anchorage</strong>. Angle<br />
Orthod 2004;74:558-67.<br />
4. Ohmae M, Saito S, Morohashi T, Seki K, Qu H, Kanomi R, et al. A<br />
clinical and histological evaluati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> titanium mini-implants as<br />
anchors for orthod<strong>on</strong>tic intrusi<strong>on</strong> in the beagle dog. Am J Orthod<br />
Dent<str<strong>on</strong>g>of</str<strong>on</strong>g>acial Orthop 2001;119:489-97.<br />
5. Park HS, Bae SM, Kyung HM, Sung JH. Micro-implant <strong>anchorage</strong><br />
for treatment <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>skeletal</strong> Class I bialveolar protrusi<strong>on</strong>. J Clin<br />
Orthod 2001;35:417-22.<br />
6. Park HS, Kyung HM, Sung JH. A simple method <str<strong>on</strong>g>of</str<strong>on</strong>g> molar uprighting<br />
with micro-implant <strong>anchorage</strong>. J Clin Orthod 2002;36:<br />
592-6.<br />
7. Lin JC, Liou EJ. A new b<strong>on</strong>e <str<strong>on</strong>g>screw</str<strong>on</strong>g> for orthod<strong>on</strong>tic <strong>anchorage</strong>.<br />
J Clin Orthod 2003;37:676-81.<br />
8. Melsen B. Mini-implants: where are we? J Clin Orthod 2005;39:<br />
539-47.<br />
9. Liou EJ, Pai BC, Lin JC. Do mini<str<strong>on</strong>g>screw</str<strong>on</strong>g>s remain stati<strong>on</strong>ary under orthod<strong>on</strong>tic<br />
forces? Am J Orthod Dent<str<strong>on</strong>g>of</str<strong>on</strong>g>acial Orthop 2004;126:42-7.<br />
10. Huja SS, Litsky AS, Beck FM, Johns<strong>on</strong> KA, Larsen PE. Pull-out<br />
strength <str<strong>on</strong>g>of</str<strong>on</strong>g> m<strong>on</strong>ocortical <str<strong>on</strong>g>screw</str<strong>on</strong>g>s placed in the maxillae and mandibles<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> dogs. Am J Orthod Dent<str<strong>on</strong>g>of</str<strong>on</strong>g>acial Orthop 2005;127:<br />
307-13.<br />
11. Melsen B, Costa A. Immediate loading <str<strong>on</strong>g>of</str<strong>on</strong>g> implants used for orthod<strong>on</strong>tic<br />
<strong>anchorage</strong>. Clin Orthod Res 2000;3:23-8.<br />
12. Cheng HC, Yen E, Chen LS, Lee ST. The analysis <str<strong>on</strong>g>of</str<strong>on</strong>g> failure cases<br />
using Orthoanchor K1 mini-implant system as orthod<strong>on</strong>tic <strong>anchorage</strong>.<br />
J Dent Res 2003;82(Spec Iss B):B-214, 1624.<br />
13. Cheng SJ, Tseng IY, Lee JJ, Kok SH. A prospective study <str<strong>on</strong>g>of</str<strong>on</strong>g> the<br />
risk factors associated with failure <str<strong>on</strong>g>of</str<strong>on</strong>g> mini-implants used for orthod<strong>on</strong>tic<br />
<strong>anchorage</strong>. Int J Oral Maxill<str<strong>on</strong>g>of</str<strong>on</strong>g>ac Implants 2004;19:<br />
100-6.<br />
14. Adell R, Lekholm U, Rockler B, Branemark P. A 15-year study <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
osseointegrated implants in the treatment <str<strong>on</strong>g>of</str<strong>on</strong>g> the edentulous jaw.<br />
Int J Oral Surg 1981;6:387-416.<br />
15. Albrektss<strong>on</strong> T, Lekholm U. Osseointegrati<strong>on</strong>: current state <str<strong>on</strong>g>of</str<strong>on</strong>g> the<br />
art. Dent Clin North Am 1989;33:537-54.<br />
16. Brettin BT, Grosland NM, Qian F, Southard KA, Stuntz TD,<br />
Morgan TA, et al. Bicortical vs m<strong>on</strong>ocortical orthod<strong>on</strong>tic <strong>skeletal</strong><br />
<strong>anchorage</strong>. Am J Orthod Dent<str<strong>on</strong>g>of</str<strong>on</strong>g>acial Orthop 2008;134:625-35.<br />
17. Miyawaki S, Koyama I, Inoue M, Mishima K, Sugahara T,<br />
Takano-Yamamoto T. Factors associated with the stability <str<strong>on</strong>g>of</str<strong>on</strong>g> titanium<br />
<str<strong>on</strong>g>screw</str<strong>on</strong>g>s placed in the posterior regi<strong>on</strong> for orthod<strong>on</strong>tic <strong>anchorage</strong>.<br />
Am J Orthod Dent<str<strong>on</strong>g>of</str<strong>on</strong>g>acial Orthop 2003;124:373-8.<br />
18. Kircelli BH, Pekta ZO, Uckan S. Orthopedic orotracti<strong>on</strong> with<br />
<strong>skeletal</strong> <strong>anchorage</strong> in a patient with maxillary hypoplasia and<br />
hypod<strong>on</strong>tia. Angle Orthod 2005;76:156-63.