Download
Download Download
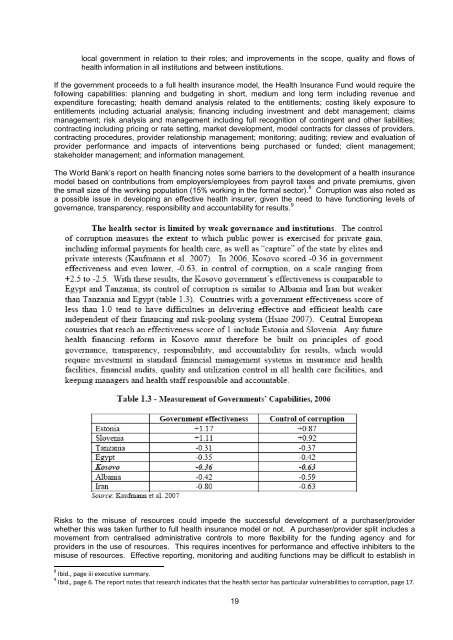
Some issues with this method of financing include: Information Lack of an integrated funding approach for health services resulting in poor links between capital and recurrent funding (a problem identified in the Master Plan), difficulties in linking funding to performance, difficulties for providers in managing resources when they are controlled by different entities, and difficulties in creating incentives for performance. Poor links between primary, secondary and tertiary care with different funders with incentives that may not always be aligned (e.g., municipalities with incentives to increase resources for their area at the expenses of others and to cost shift from primary care onto hospitals, including the University clinic, etc). Fragmented and inadequate information on health status and services provided in various institutions, making it difficult to plan, manage and monitor health services. The challenges noted in the draft Health Sector Strategy include improving the information in the health sector. A report on health financing in Kosovo noted that: 6 There is a lack of information on health outcomes, including morbidity and mortality statistics that could be used for international comparison. Kosovo does not collect data on common health indicators, including bacis demographic indicators; lifestyle- and environment-related indicators; mortality, morbidity, and disability; and health care resources comprehensive utilization, and expenditure. The existing data on the population‟s demographic characteristics and health status are highly contradictory, and highlight the need for investment in better monitoring and evaluation capacity at the MoH. This lack of data prevents analysis of trends and comparisons of international health statistics that could help to support the formulation and monitoring of health policyat the national level. Health insurance Another challenge is the preparatory work for health insurance. The report by the World Bank on health financing outlines the considerable work required to establish the foundations for such a development including: 7 Planning the reforms and providing a structure to manage and monitor them; planning needs to cover the areas outlined below and set out the transition path for these changes over time, in a feasible sequence that takes account of critical paths and capacity to undertake the reforms as well as the finances available for making the changes. Risk management strategies should be included in the reform plan. Developing the policy and drafting and putting law in place including law relating to redefined roles for a purchaser provider split; governance and accountability structure for hospitals, other providers, and the insurance or purchasing body; financing; licensing and accreditation; definition of entitlements (health care package); fees and charges; health information requirements relating to roles, use, transfer, storage, etc; prohibitions including on fees and charges; etc. Rationalisation and development of providers and other key institutions as discussed in the Master Plan and in line with requirements for progression to a health purchaser/provider split whether in the form of a health insurance model or single funder/purchaser. Capacity building in all institutions including governance of semi-autonomous institutions such as hospitals and the health insurer or purchaser/funder; developing MOH capability in policy, planning, regulation, information management, reporting, monitoring, and review; developing the purchasing/funding role whether in the insurer or MOH or other institution (discussed further below); improving management including internal financial management, information management, contracting, and many other capabilities for hospitals and other providers; developing capacity in 6 World Bank, “Kosovo Health Financing Reform Study,” page 10. 7 World Bank, “Kosovo Health Financing Reform Study,” table 7.2 page 120. 18
local government in relation to their roles; and improvements in the scope, quality and flows of health information in all institutions and between institutions. If the government proceeds to a full health insurance model, the Health Insurance Fund would require the following capabilities: planning and budgeting in short, medium and long term including revenue and expenditure forecasting; health demand analysis related to the entitlements; costing likely exposure to entitlements including actuarial analysis; financing including investment and debt management; claims management; risk analysis and management including full recognition of contingent and other liabilities; contracting including pricing or rate setting, market development, model contracts for classes of providers, contracting procedures, provider relationship management; monitoring; auditing; review and evaluation of provider performance and impacts of interventions being purchased or funded; client management; stakeholder management; and information management. The World Bank‟s report on health financing notes some barriers to the development of a health insurance model based on contributions from employers/employees from payroll taxes and private premiums, given the small size of the working population (15% working in the formal sector). 8 Corruption was also noted as a possible issue in developing an effective health insurer, given the need to have functioning levels of governance, transparency, responsibility and accountability for results. 9 Risks to the misuse of resources could impede the successful development of a purchaser/provider whether this was taken further to full health insurance model or not. A purchaser/provider split includes a movement from centralised administrative controls to more flexibility for the funding agency and for providers in the use of resources. This requires incentives for performance and effective inhibiters to the misuse of resources. Effective reporting, monitoring and auditing functions may be difficult to establish in 8 Ibid., page iii executive summary. 9 Ibid., page 6. The report notes that research indicates that the health sector has particular vulnerabilities to corruption, page 17. 19
- Page 5 and 6: 5. There are many constraints on ma
- Page 7 and 8: 9. Once the structure is decided th
- Page 9 and 10: SECTION I: Legal, policy and medium
- Page 11 and 12: Centre of Telemedicine reports to P
- Page 13 and 14: other functions it could work along
- Page 15 and 16: The whole-of-government budget proc
- Page 17 and 18: Lack of planning and policy functio
- Page 19 and 20: improve their planning and policy m
- Page 21 and 22: Structural problems with excessive
- Page 23 and 24: One option for the organisation of
- Page 25 and 26: Some issues raised by staff include
- Page 27 and 28: main providers of services funded b
- Page 29 and 30: Policy and planning unit A variatio
- Page 31 and 32: Health information is part of the D
- Page 33 and 34: Issues raised by staff and others O
- Page 35 and 36: The roles and functions of the boar
- Page 37 and 38: Some countries have combined health
- Page 39 and 40: Appendices Vertical Functional Revi
- Page 41 and 42: Valdet Hashani, Primary Health Care
- Page 43 and 44: split proposed in the World Bank re
- Page 45 and 46: 56.2. Implementation of the health
- Page 47 and 48: This law regulates tobacco products
- Page 49 and 50: Provides for a grant for minimum st
- Page 51 and 52: V. Fourth goal - Functionalize, reo
- Page 53 and 54: Health information Develop effectiv
- Page 55: Two projects on Health and Environm
- Page 59 and 60: Hospital prepares its own budget an
- Page 61 and 62: Appendix E: Number of Staff and Bud
- Page 63 and 64: Agency for the control of health ca
- Page 65 and 66: Appendix G Additional advice provid
- Page 67 and 68: Improving the health status analysi
- Page 69 and 70: 3. Accountability. Incentives and s
- Page 71 and 72: While there is clarity of central g
- Page 73 and 74: 50.2 Section 1.2 of the Law on Pubi
- Page 75 and 76: [check if section 13 is OK or are t
- Page 77 and 78: all of the directors as soon as pra
- Page 79 and 80: Template for examining decision rig
- Page 81 and 82: Name of agency Invest Give loans bu
- Page 83 and 84: Name of agency Modify a license Can
- Page 85 and 86: The issues raised at the start of t
- Page 87 and 88: Figure 2: Integrated management cyc
- Page 89: fees. The proposal could exclude th
local government in relation to their roles; and improvements in the scope, quality and flows of<br />
health information in all institutions and between institutions.<br />
If the government proceeds to a full health insurance model, the Health Insurance Fund would require the<br />
following capabilities: planning and budgeting in short, medium and long term including revenue and<br />
expenditure forecasting; health demand analysis related to the entitlements; costing likely exposure to<br />
entitlements including actuarial analysis; financing including investment and debt management; claims<br />
management; risk analysis and management including full recognition of contingent and other liabilities;<br />
contracting including pricing or rate setting, market development, model contracts for classes of providers,<br />
contracting procedures, provider relationship management; monitoring; auditing; review and evaluation of<br />
provider performance and impacts of interventions being purchased or funded; client management;<br />
stakeholder management; and information management.<br />
The World Bank‟s report on health financing notes some barriers to the development of a health insurance<br />
model based on contributions from employers/employees from payroll taxes and private premiums, given<br />
the small size of the working population (15% working in the formal sector). 8 Corruption was also noted as<br />
a possible issue in developing an effective health insurer, given the need to have functioning levels of<br />
governance, transparency, responsibility and accountability for results. 9<br />
Risks to the misuse of resources could impede the successful development of a purchaser/provider<br />
whether this was taken further to full health insurance model or not. A purchaser/provider split includes a<br />
movement from centralised administrative controls to more flexibility for the funding agency and for<br />
providers in the use of resources. This requires incentives for performance and effective inhibiters to the<br />
misuse of resources. Effective reporting, monitoring and auditing functions may be difficult to establish in<br />
8 Ibid., page iii executive summary.<br />
9 Ibid., page 6. The report notes that research indicates that the health sector has particular vulnerabilities to corruption, page 17.<br />
19


