Summer 2012 Newsletter - UCSF Helen Diller Family ...
Summer 2012 Newsletter - UCSF Helen Diller Family ...
Summer 2012 Newsletter - UCSF Helen Diller Family ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Special Interest<br />
Articles:<br />
• Hormone receptor<br />
negative breast<br />
cancer: Improving the<br />
effectiveness of<br />
chemotherapy by<br />
targeting immune<br />
cells<br />
Page 1, cont. Page 6<br />
• 5 th International<br />
Workshop on Breast<br />
Densitometry and<br />
Mammography-<br />
Based Risk<br />
Assessment<br />
Page 2<br />
• Views from an<br />
advocate: Strategies<br />
to stay sane – post<br />
treatment<br />
Pages 3<br />
• Athena Breast Health<br />
Network<br />
Page 4<br />
• Targeted Cancer<br />
Therapy Enters<br />
Phase I Clinical Trial<br />
Page 5<br />
• BOP members<br />
participate in Tri-<br />
Valley SOCKs Bras<br />
for the Cause<br />
Page 6<br />
• Going West to do<br />
some SPY-ing (article<br />
from EBCC)<br />
Page 7<br />
• BCC Volunteer<br />
Participates in<br />
American Association<br />
for Cancer Research<br />
(AACR) Scientist<br />
Survivor Program<br />
(article from Breast<br />
Cancer Connections)<br />
Page 8<br />
Editor: Karla<br />
Kerlikowske, MD<br />
Professor of<br />
Medicine,<br />
Epidemiology and<br />
Biostatistics, <strong>UCSF</strong><br />
Bay Area Breast Cancer<br />
SPORE <strong>Newsletter</strong><br />
Specialized Program of Research Excellence at the University of California San Francisco<br />
Hormone receptor negative breast cancer: Improving the<br />
effectiveness of chemotherapy by targeting immune cells<br />
By Hope Rugo, MD, Shelley Hwang, MD, and Lisa Coussens, PhD<br />
Triple-negative breast cancer (TNBC)<br />
refers to a heterogeneous group of tumors<br />
that are defined on the basis of absent<br />
hormone receptors, estrogen (ER) and<br />
progesterone (PR), as well as the HER-2<br />
receptor and protein. TNBC are often<br />
associated with worse outcome due to<br />
aggressive tumor cell activity and fewer<br />
options for effective treatment. Some of<br />
these cancers are also associated with<br />
inherited abnormalities in the BRCA<br />
genes. In the advanced disease setting,<br />
many of these tumors are fast-growing<br />
with a short duration of treatment response<br />
and rapid development of resistance to<br />
standard therapy.<br />
Breast cancer can be classified by patterns<br />
of gene expression into several subtypes,<br />
one of which is referred to as basal-like.<br />
Most but not all TNBC are categorized as<br />
basal-like, and basal-like or TNBC<br />
accounts for ~15% of breast cancer<br />
diagnoses. Compared to other breast<br />
cancers, TNBC is commonly of higher<br />
grade, occurs more frequently in younger<br />
women and those of African American<br />
descent, and is associated with an<br />
increased probability of metastasis as well<br />
as poorer survival. High treatment<br />
responses are seen when patients with<br />
TNBC are treated with primary<br />
chemotherapy before surgery and many of<br />
these women will be cured of their<br />
disease, however relapses still occur and<br />
are commonly seen within the first three<br />
years after initial diagnosis. Approximately<br />
20% of women diagnosed with early stage<br />
breast cancer will develop systemic<br />
recurrence and 5% will present at time of<br />
initial diagnosis with spread of cancer to<br />
other organs (metastatic disease). A<br />
disproportionate percent of patients with<br />
metastatic breast cancer will have TNBC.<br />
For this group, although chemotherapy is a<br />
critical component of treatment with<br />
improved cancer related symptoms and<br />
prolonged survival, all patients will<br />
eventually succumb to their disease.<br />
Improving treatment for TNBC is a critical<br />
goal of breast cancer research.<br />
While breast cancer has not historically<br />
been linked to inflammation or infection, it<br />
exhibits tumor-associated inflammation<br />
characterized by infiltration of white blood<br />
cells into developing and progressing<br />
tumors. In breast cancers, macrophages<br />
(a type of white blood cell) are the most<br />
plentiful immune cell type present.<br />
Recently, several investigators have<br />
shown that tumor-associated<br />
macrophages are independently increased<br />
in TNBC. Supporting this finding, a<br />
macrophage response gene expression<br />
signature was identified in 17-25% of<br />
breast cancers associated with low ER and<br />
PR as well as significantly worse outcome.<br />
PLX3397 is an oral agent that blocks<br />
macrophages and has been shown to be<br />
safe in humans with cancer. Compelling<br />
animal data from the laboratory of Dr. Lisa<br />
Coussens using a transgenic mouse<br />
model of mammary carcinogenesis<br />
demonstrated that treatment of late-stage<br />
Continued on Page 6
Bay Area Breast Cancer SPORE <strong>Newsletter</strong><br />
The 5 th International Workshop on Breast Densitometry<br />
and Mammography-Based Risk Assessment was held<br />
June 9-10, 2011 in San Francisco, with 160 participants<br />
representing more than 50 different institutions from<br />
around the world. Investigators attending presented<br />
research on new methods to measure breast density,<br />
genetics and biology of breast density and use of breast<br />
density in clinical practice to determine at what age to start<br />
screening mammography and how often to be screened.<br />
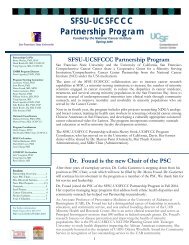
Breast density research is clinically relevant since it is one<br />
of the strongest risk factors for breast cancer. Breast<br />
density is a radiological term and that describes the<br />
relative amounts of fat, epithelial, and connective tissues<br />
that appear on a mammogram due to differences in X-ray<br />
attenuation. Fat appears radiolucent or dark, while<br />
epithelial and connective tissues are radiographically<br />
dense and appear light or white (Figure 1). When<br />
comparing women that have mostly white on their<br />
mammogram (high breast density) to those that have<br />
mostly dark (low breast density), women with high breast<br />
Page 2<br />
5 th International Workshop on Breast Densitometry and Mammography-Based<br />
Risk Assessment<br />
By Karla Kerlikowske, MD, <strong>UCSF</strong> Breast SPORE Investigator<br />
density are at 4 to 6-fold higher risk of developing breast<br />
cancer. For the purposes of this article, high breast density<br />
is defined as an amount of greater than 50% dense tissue<br />
seen on imaging. Of women undergoing mammography,<br />
32% show high density, which exceeds the prevalence of<br />
most risk factors such as family history of breast cancer.<br />
Key findings presented at the 5 th International workshop<br />
include:<br />
• Volume of breast density measured as either<br />
fibroglandular volume or percent fibroglandular volume is<br />
strongly associated with breast cancer risk and improves<br />
the accuracy of risk assessment over clinical risk factors<br />
alone.<br />
• For women aged 40 to 49 years with high breast density,<br />
and with either a first-degree relative with breast cancer<br />
or history of a prior breast biopsy, the benefits versus<br />
harms for performing mammography every two years is<br />
similar to screening an average-risk woman in her<br />
fifties every two years.<br />
• Women with fatty breasts have a decreased risk of<br />
breast cancer. Women with high breast density have<br />
decreased expression of CD36 that helps<br />
development of fat cells in the breast.<br />
• Women aged 50 to 59 years with low breast density<br />
(fatty breasts) could be screened less often than<br />
every two years.<br />
• High breast density is strongly and positively<br />
associated with breast cancer risk for several tumor<br />
subtypes including estrogen-receptor (ER) positive<br />
breast cancer, triple negative breast cancer and<br />
HER2 positive breast cancer.<br />
• rs10995190 single-nucleotide polymorphism (SNP), a<br />
DNA sequence, is associated with breast cancer risk<br />
and high breast density suggesting that the genetics<br />
of breast cancer and breast density may be linked.<br />
Figure 1: Left panel low<br />
density and right panel high<br />
breast density.<br />
• BreastCare (Breast Cancer Risk Education) study is<br />
evaluating a tablet-based intervention to increase<br />
patient knowledge about her personal breast cancer<br />
risk including factors that increase risk such as<br />
breast density, and increase patient-physician<br />
discussion of risk-reduction practices.<br />
The workshop was chaired by Drs. Karla Kerlikowske,<br />
John Shepherd and Steve Cummings and sponsored<br />
by <strong>UCSF</strong>, Daniel and Phyllis Da Costa Funds of the<br />
CPMC Foundation with contributions from the<br />
California Breast Cancer Research Program,<br />
American Cancer Society and the Matakina<br />
International Limited. The next workshop will be held in<br />
2013.
Bay Area Breast Cancer SPORE <strong>Newsletter</strong><br />
Page 3<br />
Views from an Advocate: strategies to stay sane – post treatment<br />
By Hannah Klein Connolly, Breast SPORE Advocate<br />
As a <strong>UCSF</strong> research advocate, I am<br />
often asked, “what do you do?” I was<br />
initially unclear about my role. Sure, I<br />
had done plenty of investigation on<br />
the topic of breast cancer following<br />
my own diagnosis. But, I wondered<br />
what did I truly know about the<br />
biology of cancer and the world of<br />
research; how was I to make an<br />
impact?<br />
Armed with the desire to create<br />
change, and an interest in science<br />
(keep in mind, my last science class<br />
was at least 30 years ago) and well<br />
into my own treatment, I responded to<br />
an inquiry on a bulletin board in the<br />
<strong>UCSF</strong> <strong>Helen</strong> <strong>Diller</strong> Breast Cancer<br />
Center.<br />
I had worked in breast cancer<br />
activism in the early 1990s and had<br />
designed the original breast cancer<br />
flag. Having worked with the pioneers<br />
in the activist movement from Breast<br />
Cancer Action and Breast Cancer<br />
Fund, the choice to become a<br />
research “advocate” felt natural and<br />
empowering. I would have the<br />
opportunity to speak on behalf of<br />
breast cancer patients to those<br />
studying and treating breast cancer.<br />
Simply put, research advocates are<br />
trained to advocate for the<br />
advancement of treatment for<br />
patients. Through advocacy, doctors<br />
and scientists have the ability to hear<br />
patients’ experiences and concerns.<br />
The only barrier - my lack of scientific<br />
knowledge!<br />
Still undeterred, I began attending<br />
weekly Wednesday morning Breast<br />
Oncology Program (BOP) research<br />
meetings. My mind would glaze over<br />
after an hour of listening to scientists<br />
pontificate about the ‘new downregulated<br />
receptor…’. After these<br />
meetings, I would speak with other<br />
SPORE advocates in effort to gain an<br />
understanding of these discussions. It<br />
became very apparent to me that I<br />
needed the basics. That was when I<br />
learned about NBCC’s Project LEAD,<br />
a weeklong, intensive science course<br />
about breast cancer.<br />
I was fortunate this summer to have<br />
been accepted and to have taken part<br />
in project LEAD. It was an amazing<br />
experience. Incredible professors<br />
from all over the country taught<br />
classes from early morning into the<br />
evening. We lived, breathed, and<br />
bathed biology, statistics, and breast<br />
cancer research. That amazing<br />
week’s crash course enabled me to<br />
go back to the BOP meetings and ask<br />
meaningful questions amongst the<br />
researchers.<br />
Now as a trained advocate, speaking<br />
on behalf of breast cancer patients, I<br />
can truly help these scientists find<br />
more efficient ways to collaborate and<br />
communicate as they move research<br />
from the laboratory to the clinic.<br />
Along this extended breast cancer<br />
journey, I have also had a variety<br />
of speaking opportunities. I have<br />
given presentations at the <strong>UCSF</strong><br />
Breast Oncology Program<br />
Scientific Retreat in 2011, the<br />
<strong>UCSF</strong> didactic course, Biology of<br />
Breast Cancer offered through the<br />
Department of Laboratory<br />
Medicine, the 2011 Breast Cancer<br />
SPORE External Advisory Board<br />
on behalf of the Advocacy Core,<br />
and the NCI site visit as a Patient<br />
Advocate on the Bay Area<br />
Physical Sciences and Oncology<br />
Center.<br />
What, you may ask, comes next? I<br />
will be working with the Tissue<br />
Utilization Committee helping to<br />
determine how tissue samples are<br />
to be used. I look forward to<br />
addressing pertinent issues about<br />
tissue use that are important within<br />
the patient community – after all,<br />
as a patient advocate, we are the<br />
face of breast cancer to<br />
researchers who have made it<br />
their life work to solve these<br />
complex questions!<br />
The Bay Area Breast Cancer SPORE<br />
<strong>Newsletter</strong> is produced annually by<br />
the SPORE Advocacy and Tissue &<br />
Outcomes Cores at <strong>UCSF</strong>.<br />
It is mailed to all current study<br />
participants as well as breast care<br />
surgeons, oncologists, researchers,<br />
and Breast Oncology Program<br />
Members at <strong>UCSF</strong>, CPMC and<br />
SFGH.<br />
If you have questions or comments<br />
about the material printed in this<br />
newsletter, or if you would like to have<br />
additional copies sent, please call the<br />
Outcomes Office at:<br />
(415) 353-9763.<br />
More information about SPORE and<br />
related studies, as well as archived<br />
newsletter editions, is available at:<br />
http://cancer.ucsf.edu/breast_spore
Bay Area Breast Cancer SPORE <strong>Newsletter</strong><br />
The Athena Breast Health Network<br />
Alexandra Solomon, <strong>UCSF</strong> Athena Program Manager<br />
The Athena Breast Health Network (Athena) is a unique<br />
collaboration among the five University of California (UC)<br />
medical/cancer centers (<strong>UCSF</strong>, UC Davis, UCLA, UC<br />
Irvine, and UCSD), the Graduate School of Public Health<br />
at UC Berkeley, and many other public and private<br />
partners. Athena was founded by Dr. Laura Esserman<br />
and is sponsored among others by the University of<br />
California Office of the President and the Safeway<br />
Foundation.<br />
Athena is integrating clinical care and research in order to<br />
revolutionize the delivery of breast care. By standardizing<br />
the collection of data from both patients and physicians,<br />
integrating molecular profiling of tumors at the time of<br />
breast cancer diagnosis, and creating an unparalleled<br />
biospecimen repository, Athena will enable personalized<br />
care informed by science and will fuel continuous<br />
improvement in treatment options and outcomes.<br />
Key components of Athena include:<br />
• Identifying women at high risk for breast cancer who will<br />
be offered prevention services and decision support.<br />
Page 4<br />
• A comprehensive informatics strategy that includes<br />
tools to collect, analyze and distribute clinical and<br />
research data in real time.<br />
• Web-based decision tools for patients and providers<br />
to translate clinical information into treatment options<br />
– allowing physicians to tailor treatment to biology,<br />
patient preference and clinical performance.<br />
• A data and biospecimen repository to support largescale,<br />
longitudinal studies that will enable tailored<br />
prevention and treatment strategies.<br />
Underpinning these goals is a commitment by Athena<br />
clinicians and researchers across California to share<br />
data, as well as a culture that supports continuous<br />
clinical improvement. With this unique collaboration,<br />
Athena aims to change the choices for patients today<br />
and create a better future for all women at risk of<br />
developing breast cancer.<br />
Athena started to enroll women who are coming to<br />
<strong>UCSF</strong> for their mammography screening in December<br />
2011 and will roll out in the clinic by summer of <strong>2012</strong>.
Bay Area Breast Cancer SPORE <strong>Newsletter</strong><br />
Targeted Cancer Therapy Enters Phase I Clinical Trial<br />
John Park, MD, <strong>UCSF</strong> Breast SPORE Investigator<br />
Targeted therapies have been described by many as<br />
the most promising new approach to cancer treatment,<br />
but in many cases have shown disappointing potency<br />
against cancer. In research initiated under the NCI<br />
Breast Cancer SPORE Program, we have developed a<br />
strategy that combines molecular targeting against<br />
specific types of tumors and special drug delivery<br />
capabilities that exemplifies a multifunctional<br />
nanotechnology approach to cancer treatment (1). Our<br />
Breast Cancer SPORE project involves a close<br />
collaboration with the laboratories of Drs. James D.<br />
Marks and Chris Benz as well as my lab. We have<br />
developed novel, very small particles that contain<br />
cancer drugs carried in the blood stream. These<br />
particles are called nanoparticle/liposomal agents and<br />
are directed to tumor cells via monoclonal antibody<br />
(MAb) fragments. Realization of this strategy required<br />
new antibody technologies for targeting the correct<br />
tumor cells and an advanced delivery system that<br />
could carry the drugs in the bloodstream to the tumor.<br />
This technology has yielded HER2-targeted immuneliposomal<br />
doxorubicin (HER2-targeted ILs-dox), as<br />
well as other liposomal delivery systems containing<br />
different MAbs and drugs.<br />
These drug-containing immunoliposomes bind HER2overexpressing<br />
(her-2-positive) tumors, and are then<br />
taken up by the tumor cells to damage it. These anti-<br />
HER2 immunoliposomes loaded with the<br />
chemotherapy doxorubicin display potent and selective<br />
anticancer activity against HER2-overexpressing<br />
tumors since the drug is targeted to tumor cells that<br />
overexpress HER2. This new delivery system has<br />
superior efficacy over all other treatments tested,<br />
including some of the most commonly-prescribed<br />
chemotherapies (2). Our anti-HER2 immunoliposomal<br />
doxorubicin agent is able to spare low-HER2<br />
expressing non-cancer cells, including normal heart<br />
cells (3); this may mean reduced cardiotoxicity as<br />
compared to standard chemotherapy.<br />
Page 5<br />
Clinical trials<br />
Working with the NCI Drug Development Group<br />
(DDG), we developed a procedure for manufacturing<br />
this new nanoparticle drug (4,5). We have also<br />
collaborated with industry partners for the actual GMP<br />
manufacturing, toxicology and clinical development;<br />
the many steps involved in these collaborations were<br />
long and arduous. Ultimately, the manufactured agent,<br />
called MM-302, was observed to be safe in preclinical<br />
studies, and the FDA granted an Investigational New<br />
Drug (IND) application in 2010. The multicenter Phase<br />
I clinical trial has now been initiated, and patients have<br />
begun to receive this new treatment. Patients must<br />
have HER2-positive advanced breast cancer<br />
previously treated with trastuzumab (aka, Herceptin).<br />
The trial has opened at Karmanos (Detroit, MI) and<br />
<strong>UCSF</strong>. Dr. Pamela Munster, Director of the Early<br />
Phase Clinical Trials program, leads the <strong>UCSF</strong> Phase<br />
I portion.<br />
Meanwhile, another agent developed within our<br />
SPORE research, nanoliposomal CPT-11, has just<br />
entered Phase III clinical trials for advanced pancreas<br />
cancer.<br />
The discovery of new and better cancer treatments is<br />
an important enterprise. Academic centers, with their<br />
strong basic research capabilities, must be<br />
encouraged to further innovate from initial discoveries<br />
of targets and technologies to fully translational clinical<br />
products. Concerns about declining productivity in new<br />
molecular entities and drug approvals from the<br />
pharmaceutical industry highlight the importance of<br />
“diversification” of the discovery process.<br />
REFERENCES<br />
1. Park, J.W. Nanotechnology in oncology. ASCO 2006<br />
2. Park JW, Hong K, Kirpotin DB, Colbern G, Shalaby R, Baselga J, Shao Y, Nielsen<br />
UB, Marks JD, Moore D, Papahadjopoulos D, and Benz CC. Anti-HER2<br />
immunoliposomes: enhanced anticancer efficacy due to targeted delivery. Clin.<br />
Cancer Res. 2002, 8:1172-1181.<br />
3. Wickham, T. J. et al. Preclinical safety and activity of MM-302, a HER2-targeted<br />
liposomal doxorubicin designed to have an improved safety and efficacy profile<br />
over approved anthracyclines. Proc. SABCS, [Abstract P3-14-09] (2010).<br />
4. Nellis DF, Ekstrom DL, Kirpotin DB, Zhu J, Andersson R, Broadt TL, Ouellette TF,<br />
Perkins SC, Roach JM, Drummond DC, Hong K, Marks JD, Park JW, and Giardina<br />
SL. Preclinical manufacture of an anti-HER2 scFv-PEG-DSPE, liposome-inserting<br />
conjugate. 1. Gram-scale production and purification. Biotechnol. Progress 2005,<br />
21 (1), 205 -220.<br />
5. Nellis DF, Giardina SL, Janini G, Shenoy SR, Marks JD, Tsai R, Drummond DC,<br />
Hong K, Park JW, Ouellette TF, Perkins SC, and Kirpotin DB. Preclinical<br />
manufacture of an anti-HER2 scFv-PEG-DSPE, liposome-inserting conjugate. 2.<br />
Conjugate micelle identity, purity, stability and potency analysis. Biotechnol.<br />
Progress 2005, 21 (1), 221 -232.
Bay Area Breast Cancer SPORE <strong>Newsletter</strong><br />
Hormone Receptor Negative Breast Cancer, continued<br />
tumor-bearing mice with PLX3397 in combination with<br />
the chemotherapy drug paclitaxel (Taxol) reduced<br />
macrophage infiltration as well as both primary tumor<br />
growth and lung metastasis. Based on these exciting<br />
findings, we hypothesized that blocking the function of<br />
macrophages or eradicating their presence in tumor<br />
tissue will improve outcome for women receiving<br />
chemotherapy for metastatic disease. Our Komen<br />
funded research includes 1) determining the efficacy of<br />
decreasing macrophages in combination with<br />
chemotherapy in mouse models of basal-like TNBC; 2)<br />
Outcomes Office<br />
1635 Divisadero Street<br />
San Francisco, CA 94115<br />
PHONE:<br />
(415) 353-9763<br />
FAX:<br />
(415) 353-9790<br />
EMAIL:<br />
Kelly.Bolcavage@ucsfmedctr.org<br />
Page 6<br />
identifying the immune infiltrate associated with TNBC<br />
versus other types of breast cancer to identify those<br />
most likely to respond to macrophage-targeted therapy;<br />
and 3) conducting a Phase Ib/II clinical trial testing a<br />
new chemotherapy agent, eribulin, combined with<br />
PLX3397, in women with metastatic TNBC. In addition,<br />
we are starting a phase Ib clinical trial testing the safety<br />
of PLX3397 in combination with paclitaxel (Taxol) in<br />
patients with advanced cancer, and will then study this<br />
combination in the multi-center novel neoadjuvant trial,<br />
ISPY-2.<br />
<strong>UCSF</strong> Breast Oncology Program (BOP) Participates in Tri-Valley SOCKs Bras for the<br />
Cause Walk <strong>2012</strong><br />
On Saturday, May 12 th the <strong>UCSF</strong><br />
SOCK BOPers walked a fun and<br />
exhilarating 10-Kilometers (6.2<br />
miles) at the Tri-Valley SOCK’s Bras<br />
for the Cause walk. Walkers were<br />
adorned in wildly decorated bras as<br />
they made the 10-K trek in<br />
Pleasanton. They were met by<br />
applause the entire way from<br />
hardworking volunteers, passersby,<br />
and several cars decorated in bras;<br />
one dutifully titled: the Sag Limo.<br />
The walkers concluded by passing<br />
through a path of candles lighting<br />
the way to the final evening<br />
festivities. Each light represented a<br />
family member or friend who was<br />
touched by breast cancer. Walkers<br />
found the bags they had personally<br />
commemorated and seeing that<br />
their bag was one of many was an<br />
extremely moving finish to a fun and<br />
challenging walk.<br />
The walk was organized by Tri-<br />
Valley SOCK’s (Stepping Out for<br />
Cancer Kures) an all volunteer<br />
group who raises money for breast<br />
cancer research, treatment, and<br />
education. This 501(c)(3)<br />
organization is a big supporter of<br />
the Breast Oncology Program and<br />
has made significant donations to<br />
the development program.<br />
BOP Walkers: Irene Acerbi and Juan Soto<br />
Romano, Rosemary Akhurst, Dejana<br />
Braithwaite, Lamorna Brown-Swigart, Jody<br />
and Russell Frederickson, Nicole Flores,<br />
Sarah Goins, Michelle Melisko, Miki Mori,<br />
Carol Simmons, Malinda Walker and Andy<br />
Chan, Denise Wolf, Sara Zheng.<br />
BOP Volunteers: Diana Bretzinger, Diane<br />
Heditsian, Alexandra Peck, Luika<br />
Timmerman, Laura van ‘t Veer, Eunice Zhou
Bay Area Breast Cancer SPORE <strong>Newsletter</strong><br />
From European Breast Cancer Conference: The Bulletin March 23, <strong>2012</strong> article.<br />
Featuring Laura van ‘t Veer, PhD, Bay Area Breast Cancer SPORE Principle Investigator<br />
Page 7
Bay Area Breast Cancer SPORE <strong>Newsletter</strong><br />
From Breast Cancer Connections May <strong>2012</strong><br />
<strong>Newsletter</strong>:<br />
BCC Volunteer Participates in<br />
American Association for<br />
Cancer Research (ACCR)<br />
Scientist ↔ Survivor Program<br />
By Susie Brain<br />
Page 8<br />
At the American Association for Cancer Research Annual Meeting <strong>2012</strong>: Cancer Advocates Poster Session. From left to<br />
right: Jane Perlmutter, Ph.D., Lead Advocate, I-SPY-2 Clinical Trial; Susie Brain, poster presenter;, and Laura van't Veer,<br />
Ph.D., Principal Investigator, Bay Area Breast Cancer SPORE, <strong>UCSF</strong>.<br />
I recently had the opportunity to participate in the Scientist↔Survivor Program at the American Association<br />
for Cancer Research (AACR) 103 rd Annual Meeting held in Chicago. The AACR’s Scientist↔Survivor Program<br />
(SSP) was founded in 1999 by Anna D. Barker, Ph.D., formerly Deputy Director of the National Cancer<br />
Institute and currently Director of Transformative Healthcare Networks at Arizona State University. She<br />
envisioned a program “designed to build bridges and unity among leaders of the scientific community and<br />
cancer survivors and advocacy communities worldwide.”<br />
For an advocate like myself, participating in this program provided me with the opportunity to meet other<br />
patient advocates and survivors, both from US and global cancer organizations, learn about state-of-the art<br />
cancer research, and have the opportunity to interact with scientists and clinicians. The program also<br />
included special lay-language lectures on key topics of interest and small group working sessions with<br />
science mentors.<br />
As SSP advocates, we also had the opportunity to attend many of the AACR meeting presentations including<br />
forums, award lectures, plenary, and poster sessions – all listed in a program that was over 600 pages in<br />
length! The exhibition hall featured over 400 exhibitor booths selling products ranging from specialized<br />
laboratory pipettes, to environment enrichment toys for mice, to human cells and tissues. As a first-time<br />
attendee, I was overwhelmed at the size of the event! Over 18,000 researchers from around the world<br />
attend this five-day event – it was like arriving in a mini-city – with signposts to multiple meeting rooms,<br />
lecture halls, snack bars, cafes, and even a souvenir shop! Our days were long, often beginning with 7:00<br />
AM sessions and then ending with evening events such as the Annual Reception, President’s Reception, and<br />
the Survivor-Advocate Dinner.<br />
One of the requirements for SSP participation was to present a poster at the Cancer Advocates Poster<br />
Session in the main exhibitor’s hall. For me this was a daunting project that I had to undertake prior to the<br />
meeting. Luckily, I had the support of BCC and fellow advocates, and was able to present a professional 36”<br />
X 48” poster titled “The Survivorship and Advocacy Task Force Model at Breast Cancer Connections”. I was<br />
at my poster from 2:30 PM – 5:00 PM for one day, and was amazed how quickly the time went by as I<br />
chatted with visiting scientists and advocates about its contents (see photo).<br />
The take-home message from our collective group of 27 advocates is that we are all unified in our work to<br />
find a cure for a particular cancer yet we need to support the emerging science that is looking at the<br />
commonality of genomic pathways and mutations that underlie numerous cancers and not just the organ<br />
site. We heard throughout the meeting that, in Churchill’s words, we are at the “end of the beginning” and<br />
that there is a sense of optimism that amazing progress has been made in cancer research and with multidisciplinary<br />
collaborations, including continued advocacy involvement, the future holds great promise.