A double-blind randomized controlled trial of vaginal misoprostol for ...
A double-blind randomized controlled trial of vaginal misoprostol for ...
A double-blind randomized controlled trial of vaginal misoprostol for ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
A <strong>double</strong>-<strong>blind</strong> <strong>randomized</strong> <strong>controlled</strong> <strong>trial</strong> <strong>of</strong> <strong>vaginal</strong><br />
<strong>misoprostol</strong> <strong>for</strong> cervical priming be<strong>for</strong>e outpatient<br />
hysteroscopy<br />
Akmal El-Mazny, M.D., F.I.C.S., and Nermeen Abou-Salem, M.D.<br />
Department <strong>of</strong> Obstetrics and Gynecology, Faculty <strong>of</strong> Medicine, Cairo University, Cairo, Egypt<br />
Objective: To evaluate the efficacy and safety <strong>of</strong> <strong>vaginal</strong> <strong>misoprostol</strong> <strong>for</strong> cervical priming be<strong>for</strong>e diagnostic outpatient<br />
hysteroscopy (OH) without anesthesia.<br />
Design: Double-<strong>blind</strong> <strong>randomized</strong> <strong>controlled</strong> <strong>trial</strong>.<br />
Setting: University teaching hospital.<br />
Patient(s): One hundred fifty patients requiring diagnostic OH <strong>for</strong> investigation <strong>of</strong> infertility or abnormal uterine<br />
bleeding in the reproductive age.<br />
Intervention(s): Patients were randomly allocated into two equal groups (n ¼ 75). In group I, 200 mg <strong>misoprostol</strong><br />
was inserted into the posterior <strong>vaginal</strong> <strong>for</strong>nix 3 hours be<strong>for</strong>e OH; in group II (control), <strong>vaginal</strong> examination was<br />
per<strong>for</strong>med without <strong>misoprostol</strong> administration. A rigid 30 4-mm hysteroscope was used in the vaginoscopic<br />
technique.<br />
Main Outcome Measure(s): Ease <strong>of</strong> cervical entry (Likert scale), procedural time, patient acceptability (Likert<br />
scale), and pain scoring (visual analog scale).<br />
Result(s): Vaginal <strong>misoprostol</strong> significantly facilitated the procedure; cervical entry was easier, procedural time<br />
was shorter, patient acceptability was higher, and pain scoring was lower in group I compared with group II.<br />
Side effects <strong>of</strong> <strong>misoprostol</strong> were infrequent, minor, and transient. No complications were reported.<br />
Conclusion(s): The regimen <strong>of</strong> 200 mg <strong>vaginal</strong> <strong>misoprostol</strong> administered 3 hours be<strong>for</strong>e diagnostic OH is a simple,<br />
effective, and safe method <strong>of</strong> cervical priming to facilitate the procedure without anesthesia. (Fertil SterilÒ 2011;96:<br />
962–5. Ó2011 by American Society <strong>for</strong> Reproductive Medicine.)<br />
Key Words: Misoprostol, cervical priming, outpatient hysteroscopy<br />
Hysteroscopy is considered the ‘‘gold standard’’ <strong>for</strong> diagnosing intrauterine<br />
pathology (1). With the invention <strong>of</strong> the miniature hysteroscope,<br />
it is possible to per<strong>for</strong>m hysteroscopy in an <strong>of</strong>fice<br />
setting (outpatient hysteroscopy [OH]) without anesthesia <strong>for</strong> diagnostic<br />
indications and certain operative procedures (2). However,<br />
the experience <strong>of</strong> pain related to the procedure can be a major limitation<br />
<strong>for</strong> OH as a standard <strong>of</strong> care (3). This is <strong>of</strong>ten caused by the<br />
diameter <strong>of</strong> the hysteroscope and/or cervical resistance (4).<br />
Several alternatives have been proposed to per<strong>for</strong>m the procedure<br />
with an acceptable patient compliance. Local anesthetic reduces the<br />
pain experienced by women during OH. This occurs with paracervical<br />
and intracervical injections <strong>of</strong> anesthetic but not with transcervical<br />
and topical application; paracervical injection seems to be the<br />
most effective method <strong>of</strong> administering local anesthetic <strong>for</strong> the procedure<br />
(5). Nevertheless, the injection <strong>of</strong> paracervical anesthetic<br />
may cause pain and bleeding (6).<br />
Cervical priming refers to dilating or s<strong>of</strong>tening <strong>of</strong> the cervix by<br />
mechanical (e.g., laminaria) or medical (e.g., prostaglandins) means<br />
be<strong>for</strong>e an intervention in pregnant (cervical ripening) or nonpregnant<br />
women (7). Misoprostol is a synthetic analogue <strong>of</strong> prostaglandin<br />
E1 which can be given orally, <strong>vaginal</strong>ly, sublingually, buccally,<br />
or rectally (8). There is evidence supporting the use <strong>of</strong> <strong>misoprostol</strong><br />
Received February 15, 2011; revised March 28, 2011; accepted April 8,<br />
2011.<br />
A.E-M. has nothing to disclose. N.A-S. has nothing to disclose.<br />
Reprint requests: Akmal El-Mazny, M.D., F.I.C.S., Department <strong>of</strong> Obstetrics<br />
and Gynecology, Faculty <strong>of</strong> Medicine, Cairo University, Cairo, Egypt<br />
(E-mail: dr_akmalelmazny@yahoo.com).<br />
962<br />
as a cervical priming agent be<strong>for</strong>e some gynecologic procedures,<br />
such as intrauterine device insertion (9) and hysteroscopy (10).<br />
The objective <strong>of</strong> the present study was to evaluate the efficacy and<br />
safety <strong>of</strong> <strong>vaginal</strong> <strong>misoprostol</strong> <strong>for</strong> cervical priming to facilitate the<br />
procedure <strong>of</strong> diagnostic OH without the use <strong>of</strong> anesthesia, in patients<br />
with infertility or abnormal uterine bleeding (AUB).<br />
MATERIALS AND METHODS<br />
This <strong>double</strong>-<strong>blind</strong> <strong>randomized</strong> <strong>controlled</strong> <strong>trial</strong> was conducted at the<br />
OH Clinic <strong>of</strong> the Department <strong>of</strong> Obstetrics and Gynecology, Faculty<br />
<strong>of</strong> Medicine, Cairo University, from August 2009 to January 2011.<br />
The study population consisted <strong>of</strong> 150 patients requiring a diagnostic<br />
OH <strong>for</strong> investigation <strong>of</strong> infertility or AUB in the reproductive age.<br />
The study protocol was approved by the Scientific Research Committee<br />
<strong>of</strong> the department, and in<strong>for</strong>med consent was obtained<br />
from each <strong>of</strong> the patients.<br />
The exclusion criteria included: 1) contraindications to OH—<br />
marked cervical stenosis, recent or current pelvic inflammatory<br />
disease, known cervical malignancy, pregnancy, pr<strong>of</strong>use uterine<br />
bleeding, or recent uterine per<strong>for</strong>ation; 2) contraindications to prostaglandins—known<br />
sensitivity to prostaglandins, cardiovascular<br />
disease, hypertension, severe bronchial asthma, renal failure, or<br />
glaucoma; 3) previous cesarean delivery; 4) previous cervical surgery;<br />
and 5) neurologic disorders affecting the evaluation <strong>of</strong> pain.<br />
The patients were allocated into two groups with a ratio <strong>of</strong> 1:1 by<br />
using computer-generated random numbers: group I (<strong>misoprostol</strong><br />
group) and group II (control group). The patients were <strong>blind</strong>ed to<br />
group allocation. All patients underwent <strong>vaginal</strong> examination 3<br />
Fertility and Sterility â Vol. 96, No. 4, October 2011 0015-0282/$36.00<br />
Copyright ª2011 American Society <strong>for</strong> Reproductive Medicine, Published by Elsevier Inc. doi:10.1016/j.fertnstert.2011.04.049
hours be<strong>for</strong>e OH. In group I, 200 mg <strong>misoprostol</strong> (Misotac; Sigma<br />
Pharm) moistened with saline solution was inserted into the posterior<br />
<strong>for</strong>nix during the examination; in group II, the <strong>vaginal</strong> examination<br />
was per<strong>for</strong>med without <strong>misoprostol</strong> administration (no placebo<br />
was needed).<br />
All patients underwent postmenstrual OH between days 7 and 11<br />
<strong>of</strong> the cycle (except in patients with irregular bleeding). The operator<br />
per<strong>for</strong>ming the procedure was <strong>blind</strong>ed to group allocation. A<br />
rigid 30 4-mm hysteroscope (Karl Storz Endoscopy) was used<br />
without anesthesia or analgesia. The uterine cavity was distended<br />
with normal saline solution at a pressure <strong>of</strong> 100–120 mm Hg. The<br />
vaginoscopic ‘‘no touch’’ technique was followed; no speculum or<br />
tenaculum was used.<br />
The main outcome measures included: 1) ease <strong>of</strong> entry <strong>of</strong> the<br />
OH into the cervix recorded on a 5-point Likert scale (11): very<br />
difficult ¼ 1, difficult ¼ 2, fair ¼ 3, easy ¼ 4, and very easy ¼ 5;<br />
2) procedural time from introduction <strong>of</strong> the OH through the external<br />
cervical os and the visualization <strong>of</strong> the uterine cavity; 3) patient acceptability<br />
recorded by the patient on a 5-point Likert scale; 4) pain<br />
scoring recorded by the patient on a 10-point visual analog scale<br />
(VAS) (12); 5) side effects <strong>of</strong> <strong>misoprostol</strong>; and 6) complications<br />
<strong>of</strong> OH.<br />
Statistical Analysis<br />
Continuous data were expressed as mean SD and compared by using<br />
the Student t test. Categorical data were expressed as n (%) and<br />
compared by using the chi-square test or Fisher exact test as appropriate.<br />
All reported P values are two tailed, and the level <strong>of</strong> statistical<br />
significance was .05. Data analysis was per<strong>for</strong>med by using the Statistical<br />
Package <strong>for</strong> the Social Sciences, v16.0 (SPSS).<br />
RESULTS<br />
The study population consisted <strong>of</strong> 150 patients allocated into two<br />
groups: group I (<strong>misoprostol</strong> group; 75 patients) and group II (control<br />
group; 75 patients). There was no statistically significant difference<br />
in the clinical characteristics (age, gravidity, parity, and<br />
nulliparous rate) between the two groups. The indications <strong>of</strong> hysteroscopy<br />
(primary infertility, secondary infertility, and AUB)<br />
were also not significantly different (Table 1).<br />
The use <strong>of</strong> <strong>vaginal</strong> <strong>misoprostol</strong> significantly facilitated the<br />
procedure <strong>of</strong> OH. Cervical entry (Likert scale) was easier in group<br />
I (3.47 1.05) than in group II (2.93 1.02): P¼.002. Procedural<br />
time (minutes) from introduction <strong>of</strong> the OH through the external cervical<br />
os and the visualization <strong>of</strong> the uterine cavity was shorter in<br />
group I (1.95 0.47) than in group II (2.48 0.56): P
TABLE 2<br />
Main outcome measures.<br />
Variable Group I: <strong>misoprostol</strong> (n [ 75) Group II: control (n [ 75) P value<br />
Ease <strong>of</strong> cervical entry a<br />
3.47 1.05 2.93 1.02 .002<br />
Procedural time (min) 1.95 0.47 2.48 0.56 < .001<br />
Patient acceptability a<br />
2.87 0.96 2.51 0.89 .019<br />
Pain scoring b<br />
3.26 1.56 4.87 1.79 < .001<br />
Note: Values presented as mean SD.<br />
a<br />
According to 5-point Likert scale.<br />
b<br />
According to 10-point visual analog scale.<br />
El-Mazny. Misoprostol be<strong>for</strong>e <strong>of</strong>fice hysteroscopy. Fertil Steril 2011.<br />
dilatation, but it has increased side effects, mainly diarrhea and shivering<br />
(16).<br />
In agreement with our results, Sordia-Hernandez et al. (17) reported<br />
that <strong>vaginal</strong> <strong>misoprostol</strong> at a dose <strong>of</strong> 200 mg inserted 12 hours<br />
apart, starting 24 hours be<strong>for</strong>e OH without anesthesia <strong>for</strong> investigation<br />
<strong>of</strong> infertility, considerably reduces pain and the time needed <strong>for</strong><br />
hysteroscopy compared with oral <strong>misoprostol</strong> administration and<br />
placebo. They reported only one patient with nausea and two patients<br />
with referred abdominal pain in the <strong>vaginal</strong> <strong>misoprostol</strong> group<br />
(n ¼ 20). Choksuchat et al. (18) also found that 200 mg <strong>vaginal</strong> <strong>misoprostol</strong><br />
12 hours be<strong>for</strong>e conventional diagnostic hysteroscopy had<br />
efficacy similar to 400 mg oral <strong>misoprostol</strong> <strong>for</strong> cervical ripening,<br />
with less side effects.<br />
Darwish et al. (19) reported that 200 mg intra<strong>vaginal</strong> <strong>misoprostol</strong><br />
and endocervical laminaria were equally effective in inducing<br />
proper cervical priming be<strong>for</strong>e operative hysteroscopy in patients<br />
with diagnosed intrauterine lesions. Nevertheless, they observed<br />
that <strong>misoprostol</strong> may be superior, owing to easy application, reduced<br />
cost, and patient convenience and acceptability. Preutthipan et al.<br />
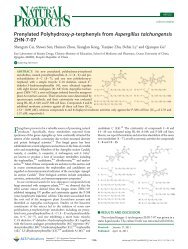
FIGURE 1<br />
Main outcome measures.<br />
10<br />
9<br />
8<br />
7<br />
6<br />
5<br />
4<br />
3<br />
2<br />
1<br />
0<br />
3.47<br />
2.93<br />
Ease <strong>of</strong> cervical entry<br />
(Likert scale)<br />
El-Mazny. Misoprostol be<strong>for</strong>e <strong>of</strong>fice hysteroscopy. Fertil Steril 2011.<br />
1.95<br />
Group I: <strong>misoprostol</strong><br />
Group II: control<br />
2.48<br />
(20) also found that <strong>vaginal</strong> <strong>misoprostol</strong> is more effective than dinoprostone<br />
<strong>for</strong> cervical priming in nulliparous women be<strong>for</strong>e hysteroscopic<br />
surgery. Although more side effects were observed in the<br />
<strong>misoprostol</strong>-treated patients, they were mild.<br />
Batukan et al. (21) reported that 400 mg <strong>vaginal</strong> <strong>misoprostol</strong> 10–<br />
12 hours be<strong>for</strong>e operative hysteroscopy is more effective than the<br />
oral route <strong>for</strong> preoperative cervical ripening in premenopausal<br />
women. Da Costa et al. (22) also found that 200 mg <strong>of</strong> <strong>vaginal</strong> <strong>misoprostol</strong><br />
reduced pain severity during diagnostic hysteroscopy in<br />
postmenopausal women. However, Oppegaard et al. (23) concluded<br />
that 1,000 mg <strong>vaginal</strong> <strong>misoprostol</strong> 12 hours be<strong>for</strong>e operative hysteroscopy<br />
has a significant cervical ripening effect compared with placebo<br />
in premenopausal but not postmenopausal women.<br />
In contrast to our results, Fernandez et al. (24) found that <strong>vaginal</strong><br />
<strong>misoprostol</strong> applied 4 hours be<strong>for</strong>e operative hysteroscopy<br />
in premenopausal women, at three different doses (200, 400, or<br />
800 mg), did not reduce the need <strong>for</strong> cervical dilatation, did not<br />
facilitate hysteroscopic surgery, and increased preoperative pain.<br />
Valente et al. (25) also observed that with the dose used in their<br />
2.87<br />
2.51<br />
Procedural time (min) Patient acceptability<br />
(Likert scale)<br />
3.26<br />
4.87<br />
Pain scoring (visual<br />
analogue scale)<br />
964 El-Mazny and Abou-Salem Misoprostol be<strong>for</strong>e <strong>of</strong>fice hysteroscopy Vol. 96, No. 4, October 2011
TABLE 3<br />
Side effects.<br />
Variable Group I: <strong>misoprostol</strong> (n [ 75) Group II: control (n [ 75) P value<br />
Nausea 7 (9.3) 2 (2.7) .166<br />
Vomiting 2 (2.7) 0 (0.0) .497<br />
Abdominal pain 6 (8.0) 4 (5.3) .745<br />
Diarrhea 4 (5.3) 1 (1.3) .367<br />
Fever 3 (4.0) 0 (0.0) .245<br />
Shivering 3 (4.0) 1 (1.3) .620<br />
Note: Values presented n (%).<br />
El-Mazny. Misoprostol be<strong>for</strong>e <strong>of</strong>fice hysteroscopy. Fertil Steril 2011.<br />
study (400 mg); <strong>vaginal</strong> <strong>misoprostol</strong> induced <strong>vaginal</strong> bleeding and<br />
precluded diagnostic anesthesia-free hysteroscopy in patients <strong>of</strong> reproductive<br />
age. Singh et al. (26) found that 400 mg <strong>vaginal</strong> <strong>misoprostol</strong><br />
4–6 hours be<strong>for</strong>e diagnostic hysteroscopy did not facilitate<br />
cervical dilation. Although it did effect a reduction in pain scores,<br />
there was no difference in patient satisfaction, need <strong>for</strong> analgesia,<br />
or sedation.<br />
REFERENCES<br />
1. Birinyi L, Darago P,T€or€ok P, Csiszar P, Major T,<br />
Borsos A, et al. Predictive value <strong>of</strong> hysteroscopic examination<br />
in intrauterine abnormalities. Eur J Obstet<br />
Gynecol Reprod Biol 2004;115:75–9.<br />
2. Bettocchi S, Ceci O, Nappi L, di Venere R,<br />
Masciopinto V, Pansini V, et al. Operative <strong>of</strong>fice hysteroscopy<br />
without anesthesia: analysis <strong>of</strong> 4863 cases<br />
per<strong>for</strong>med with mechanical instruments. J Am Assoc<br />
Gynecol Laparosc 2004;11:59–61.<br />
3. De Iaco P, Marabini A, Stefanetti M, Del Vecchio C,<br />
Bovicelli L. Acceptability and pain <strong>of</strong> outpatient hysteroscopy.<br />
JAm Assoc Gynecol Laparosc 2000;7:71–5.<br />
4. Campo R, Molinas CR, Rombauts L, Mestdagh G,<br />
Lauwers M, Braekmans P, et al. Prospective multicentre<br />
<strong>randomized</strong> <strong>controlled</strong> <strong>trial</strong> to evaluate factors<br />
influencing the success rate <strong>of</strong> <strong>of</strong>fice diagnostic hysteroscopy.<br />
Hum Reprod 2005;20:258–63.<br />
5. Cooper NA, Khan KS, Clark TJ. Local anaesthesia <strong>for</strong><br />
pain control during outpatient hysteroscopy: systematic<br />
review and meta-analysis. BMJ 2010;340:c1130.<br />
6. Vercellini P, Colombo A, Munro F, Oldani S,<br />
Bramante T, Crosignani PG. Paracervical anesthesia<br />
<strong>for</strong> outpatient hysteroscopy. Fertil Steril<br />
1995;64:221–2.<br />
7. Weeks AD, Alfirevic Z, Faundes A, H<strong>of</strong>meyr J,<br />
Safar P, Wing D. Misoprostol <strong>for</strong> induction <strong>of</strong> labor<br />
with a live fetus. Int J Gynecol Obstet<br />
2007;99:S194–7.<br />
8. Faundes A, Weeks A. Misoprostol in obstetrics and<br />
gynecology. Int J Gynecol Obstet 2007;99:S156–9.<br />
9. S€a€av I, Aronsson A, Marions L, Stephansson O,<br />
Gemzell-Danielsson K. Cervical priming with sublingual<br />
<strong>misoprostol</strong> prior to insertion <strong>of</strong> an intrauterine<br />
device in nulliparous women: a <strong>randomized</strong><br />
<strong>controlled</strong> <strong>trial</strong>. Hum Reprod 2007;22:2647–52.<br />
Fertility and Sterility â<br />
10. Crane JM, Healey S. Use <strong>of</strong> <strong>misoprostol</strong> be<strong>for</strong>e hysteroscopy:<br />
a systematic review. J Obstet Gynaecol<br />
Can 2006;28:373–9.<br />
11. Likert R. A technique <strong>for</strong> the measurement <strong>of</strong> attitudes.<br />
Arch Psychol 1932;140:1–55.<br />
12. Huskisson EC. Measurement <strong>of</strong> pain. Lancet<br />
1974;2:1127–31.<br />
13. Cooper JM, Brady RM. Hysteroscopy in the management<br />
<strong>of</strong> abnormal uterine bleeding. Obstet Gynecol<br />
Clin North Am 1999;26:217–36.<br />
14. El-Mazny A, Abou-Salem N, El-Sherbiny W,<br />
Saber W. Outpatient hysteroscopy: a routine investigation<br />
be<strong>for</strong>e assisted reproductive techniques? Fertil<br />
Steril 2011;95:272–6.<br />
15. Yang J, Vollenhoven B. Pain control in outpatient<br />
hysteroscopy. Obstet Gynecol Surv 2002;57:693–<br />
702.<br />
16. Singh K, Fong YF, Prasad RN, Dong F. Randomized<br />
<strong>trial</strong> to determine optimal dose <strong>of</strong> <strong>vaginal</strong> <strong>misoprostol</strong><br />
<strong>for</strong> preabortion cervical priming. Obstet Gynecol<br />
1998;92:795–8.<br />
17. Sordia-Hernandez LH, Rosales-Tristan E, Vazquez-<br />
Mendez J, Merino M, Iglesias JL, Garza-Leal JG,<br />
et al. Effectiveness <strong>of</strong> <strong>misoprostol</strong> <strong>for</strong> <strong>of</strong>fice hysteroscopy<br />
without anesthesia in infertile patients. Fertil<br />
Steril 2011;95:759–61.<br />
18. Choksuchat C, Cheewadhanaraks S, Getpook C,<br />
Wootipoom V, Dhanavoravibul K. Misoprostol <strong>for</strong><br />
cervical ripening in nonpregnant women: a <strong>randomized</strong><br />
<strong>double</strong>-<strong>blind</strong> <strong>controlled</strong> <strong>trial</strong> <strong>of</strong> oral versus <strong>vaginal</strong><br />
regimens. Hum Reprod 2006;21:2167–70.<br />
19. Darwish AM, Ahmad AM, Mohammad AM. Cervical<br />
priming prior to operative hysteroscopy: a <strong>randomized</strong><br />
comparison <strong>of</strong> laminaria versus <strong>misoprostol</strong>.<br />
Hum Reprod 2004;19:2391–4.<br />
In conclusion, our results indicate that the use <strong>of</strong> <strong>vaginal</strong> <strong>misoprostol</strong><br />
as a cervical priming agent is a simple method to facilitate<br />
the procedure <strong>of</strong> diagnostic OH without anesthesia in patients<br />
with infertility or AUB. Reduction <strong>of</strong> <strong>misoprostol</strong> dosage (200 mg)<br />
with shortening <strong>of</strong> the time interval between <strong>misoprostol</strong> administration<br />
and the procedure (3 hours) has been proven to be an effective<br />
regimen with minimal side effects.<br />
20. Preutthipan S, Herabutya Y. A <strong>randomized</strong> comparison<br />
<strong>of</strong> <strong>vaginal</strong> <strong>misoprostol</strong> and dinoprostone <strong>for</strong> cervical<br />
priming in nulliparous women be<strong>for</strong>e<br />
operative hysteroscopy. Fertil Steril 2006;86:990–4.<br />
21. Batukan C, Ozgun MT, Ozcelik B, Aygen E, Sahin Y,<br />
Turkylmaz C. Cervical ripening be<strong>for</strong>e operative hysteroscopy<br />
in premenopausal women: a <strong>randomized</strong>,<br />
<strong>double</strong>-<strong>blind</strong>, placebo <strong>controlled</strong> comparison <strong>of</strong> <strong>vaginal</strong><br />
and oral <strong>misoprostol</strong>. Fertil Steril 2008;89:966–73.<br />
22. da Costa AR, Pinto-Neto AM, Amorim M, Paiva LH,<br />
Scavuzzi A, Schettini J. Use <strong>of</strong> <strong>misoprostol</strong> prior to<br />
hysteroscopy in postmenopausal women: a <strong>randomized</strong>,<br />
placebo-<strong>controlled</strong> clinical <strong>trial</strong>. J Minim Invasive<br />
Gynecol 2008;15:67–73.<br />
23. Oppegaard KS, Nesheim BI, Istre O, Qvigstad E.<br />
Comparison <strong>of</strong> self-administered <strong>vaginal</strong> <strong>misoprostol</strong><br />
versus placebo <strong>for</strong> cervical ripening prior to operative<br />
hysteroscopy using a sequential <strong>trial</strong> design. BJOG<br />
2008;115:663.e1–9.<br />
24. Fernandez H, Alby JD, Tournoux C, Chauveaud-<br />
Lambling A, de Tayrac R, Frydman R, et al. Vaginal<br />
<strong>misoprostol</strong> <strong>for</strong> cervical ripening be<strong>for</strong>e operative<br />
hysteroscopy in pre-menopausal women: a <strong>double</strong><strong>blind</strong>,<br />
placebo-<strong>controlled</strong> <strong>trial</strong> with three dose regimens.<br />
Hum Reprod 2004;19:1618–21.<br />
25. Valente EP, de Amorim MM, Costa AA, de<br />
Miranda DV. Vaginal <strong>misoprostol</strong> prior to diagnostic<br />
hysteroscopy in patients <strong>of</strong> reproductive age: a <strong>randomized</strong><br />
clinical <strong>trial</strong>. J Minim Invasive Gynecol<br />
2008;15:452–8.<br />
26. Singh N, Ghosh B, Naha M, Mittal S. Vaginal <strong>misoprostol</strong><br />
<strong>for</strong> cervical priming prior to diagnostic hysteroscopy—efficacy,<br />
safety and patient satisfaction:<br />
a <strong>randomized</strong> <strong>controlled</strong> <strong>trial</strong>. Arch Gynecol Obstet<br />
2009;279:37–40.<br />
965