Physiologic and Supraphysiologic Increases in Lipoprotein Lipids ...
Physiologic and Supraphysiologic Increases in Lipoprotein Lipids ...
Physiologic and Supraphysiologic Increases in Lipoprotein Lipids ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Physiologic</strong> <strong>and</strong> supraphysiologic <strong>in</strong>creases <strong>in</strong> lipoprote<strong>in</strong> lipids <strong>and</strong> apoprote<strong>in</strong>s <strong>in</strong> late<br />
pregnancy <strong>and</strong> postpartum. Possible markers for the diagnosis of "prelipemia".<br />
A Montes, C E Walden, R H Knopp, M Cheung, M B Chapman <strong>and</strong> J J Albers<br />
Arterioscler Thromb Vasc Biol. 1984;4:407-417<br />
doi: 10.1161/01.ATV.4.4.407<br />
Arteriosclerosis, Thrombosis, <strong>and</strong> Vascular Biology is published by the American Heart Association, 7272 Greenville<br />
Avenue, Dallas, TX 75231<br />
Copyright © 1984 American Heart Association, Inc. All rights reserved.<br />
Pr<strong>in</strong>t ISSN: 1079-5642. Onl<strong>in</strong>e ISSN: 1524-4636<br />
The onl<strong>in</strong>e version of this article, along with updated <strong>in</strong>formation <strong>and</strong> services, is located on the<br />
World Wide Web at:<br />
http://atvb.ahajournals.org/content/4/4/407<br />
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles orig<strong>in</strong>ally published <strong>in</strong><br />
Arteriosclerosis, Thrombosis, <strong>and</strong> Vascular Biology can be obta<strong>in</strong>ed via RightsL<strong>in</strong>k, a service of the Copyright<br />
Clearance Center, not the Editorial Office. Once the onl<strong>in</strong>e version of the published article for which permission<br />
is be<strong>in</strong>g requested is located, click Request Permissions <strong>in</strong> the middle column of the Web page under Services.<br />
Further <strong>in</strong>formation about this process is available <strong>in</strong> the Permissions <strong>and</strong> Rights Question <strong>and</strong> Answerdocument.<br />
Repr<strong>in</strong>ts: Information about repr<strong>in</strong>ts can be found onl<strong>in</strong>e at:<br />
http://www.lww.com/repr<strong>in</strong>ts<br />
Subscriptions: Information about subscrib<strong>in</strong>g to Arteriosclerosis, Thrombosis, <strong>and</strong> Vascular Biology is onl<strong>in</strong>e<br />
at:<br />
http://atvb.ahajournals.org//subscriptions/<br />
Downloaded from<br />
http://atvb.ahajournals.org/ by guest on June 29, 2013
<strong>Physiologic</strong> <strong>and</strong> <strong>Supraphysiologic</strong> <strong>Increases</strong><br />
<strong>in</strong> Lipoprote<strong>in</strong> <strong>Lipids</strong> <strong>and</strong> Apoprote<strong>in</strong>s<br />
<strong>in</strong> Late Pregnancy <strong>and</strong> Postpartum<br />
Possible Markers for the Diagnosis of "Prelipemia"<br />
Agust<strong>in</strong> Montes, Carolyn E. Walden, Robert H. Knopp, Marian Cheung,<br />
Margaret B. Chapman, <strong>and</strong> John J. Albers<br />
A supraphysiologic (>95th percentile) rise <strong>in</strong> plasma lipids <strong>in</strong> pregnancy may serve<br />
as a marker for "prelipemia" <strong>in</strong> the same way that gestational diabetes is a marker for<br />
prediabetes. To qualify as prelipemic, subjects with an abnormal lipid rise antepartum<br />
must return to normal postpartum but may have other identify<strong>in</strong>g characteristics. This<br />
paper describes the antepartum-postpartum changes of lipoprote<strong>in</strong> lipids <strong>and</strong> apoprote<strong>in</strong>s<br />
at 34 to 38 weeks of gestation <strong>and</strong> 6 <strong>and</strong> 20 weeks postpartum <strong>in</strong> 23 subjects<br />
with physiologic <strong>and</strong> six subjects with supraphysiologic plasma lipid <strong>in</strong>creases dur<strong>in</strong>g<br />
pregnancy. These results are compared to measurements <strong>in</strong> 23 nonpregnant<br />
controls matched for weight, age, <strong>and</strong> race. In subjects with a physiologic antepartum<br />
lipid rise, postpartum total triglyceride <strong>and</strong> very low density lipoprote<strong>in</strong> (VLDL) lipids<br />
(cholesterol <strong>and</strong> triglyceride) <strong>and</strong> apo B returned to basel<strong>in</strong>e with<strong>in</strong> 6 weeks. In contrast,<br />
low density lipoprote<strong>in</strong> (LDL) showed a slow postpartum decl<strong>in</strong>e <strong>in</strong> lipids <strong>and</strong><br />
apo B with elevations rema<strong>in</strong><strong>in</strong>g at 20 weeks postpartum. High density lipoprote<strong>in</strong><br />
(HDL) cholesterol concentrations, elevated <strong>in</strong> pregnancy, rema<strong>in</strong>ed elevated at 6<br />
weeks postpartum, but fell to basel<strong>in</strong>e by 20 weeks postpartum. HDL triglyceride <strong>and</strong><br />
apo A-l concentrations, both elevated <strong>in</strong> pregnancy, returned to basel<strong>in</strong>e by 6 weeks<br />
postpartum. A supraphysiologic triglyceride rise <strong>in</strong> pregnancy was associated with a<br />
slower return of total triglycerides <strong>and</strong> VLDL to basel<strong>in</strong>e, reduced HDL cholesterol<br />
ante- <strong>and</strong> postpartum, atypical changes <strong>in</strong> LDL cholesterol dur<strong>in</strong>g pregnancy <strong>and</strong><br />
postpartum, <strong>and</strong> evidence of hyperlipidemia among family members. Two subjects<br />
with hypercholesterolemia <strong>in</strong> the nonpregnant state showed no marked exaggeration<br />
of total or LDL cholesterol concentrations <strong>in</strong> pregnancy. The data support the hypothesis<br />
that a supraphysiologic rise <strong>in</strong> plasma triglyceride concentrations <strong>in</strong> late pregnancy<br />
may serve as a marker of prelipemia. Proof of the hypothesis requires further<br />
<strong>in</strong>vestigation <strong>and</strong> longer follow-up.<br />
(Arteriosclerosis 4:407-417, July/August 1984)<br />
Glucose <strong>in</strong>tolerance <strong>and</strong> hyperlipidemia are physiologic<br />
accompaniments of normal pregnancy.<br />
12 With respect to glucose homeostasis, it is well<br />
known that some women manifest overt diabetes<br />
under the stress of pregnancy but revert to normal<br />
after delivery. The deterioration of glucose homeo-<br />
From the Northwest Lipid Research Cl<strong>in</strong>ic <strong>and</strong> the Department<br />
of Medic<strong>in</strong>e, School of Medic<strong>in</strong>e, University of Wash<strong>in</strong>gton, <strong>and</strong><br />
the Department of Biostatistics, School of Public Health <strong>and</strong> Community<br />
Medic<strong>in</strong>e, Seattle, Wash<strong>in</strong>gton.<br />
This work was supported by the Lipid Research Cl<strong>in</strong>ic Program<br />
Contract HL 12157 <strong>and</strong> Grant HD 08960 <strong>and</strong> by the Council for<br />
Tobacco Research, USA. Dr. Albers is an Established Investigator<br />
of the American Heart Association.<br />
Current address for Dr. Montes: Catedra 2, de Fisiologia, Facultad<br />
de Medic<strong>in</strong>a, Cuidad Universitaria, Madrid 3, Spa<strong>in</strong>.<br />
Address for repr<strong>in</strong>ts: Robert H. Knopp, M.D., 326 N<strong>in</strong>th Avenue,<br />
Seattle, Wash<strong>in</strong>gton 98104.<br />
Received August 17, 1983; revision accepted March 14, 1984.<br />
407<br />
stasis <strong>in</strong> pregnancy, known as gestational diabetes,<br />
134 is considered to be a form of prediabetes<br />
because it predicts later progression to overt diabetes<br />
with a high degree of accuracy. 4 It is not yet<br />
known if a similar deterioration of lipid homeostasis<br />
occurs <strong>in</strong> pregnancy, reverts to normal postpartum,<br />
<strong>and</strong> predicts the appearance of overt nongestational<br />
hyperlipidemia years later. Such a condition might be<br />
termed "prelipemia" <strong>and</strong> if identified would provide<br />
an important tool to study the natural history of hyperlipidemia<br />
from its earliest stages.<br />
This paper presents <strong>in</strong>formation to support the<br />
hypothesis that prelipemia is identified by a supraphysiologic<br />
lipid rise <strong>in</strong> pregnancy. The postpartum<br />
return of plasma lipids <strong>and</strong> lipoprote<strong>in</strong>s to basel<strong>in</strong>e is<br />
described <strong>in</strong> normal subjects. These results are compared<br />
to women with supraphysiologic elevations <strong>in</strong><br />
triglyceride or cholesterol <strong>in</strong> pregnancy but with de-<br />
Downloaded from<br />
http://atvb.ahajournals.org/ by guest on June 29, 2013
408 ARTERIOSCLEROSIS VOL 4, No 4, JULY/AUGUST 1984<br />
monstrable normolipidemia before or after pregnancy.<br />
Relatives of these subjects were exam<strong>in</strong>ed for<br />
evidence of familial hyperlipidemia. The dist<strong>in</strong>ction<br />
between physiologic <strong>and</strong> supraphysiologic antepartum<br />
<strong>in</strong>creases <strong>in</strong> lipoprote<strong>in</strong> lipids <strong>in</strong> pregnancy was<br />
made on the basis of the 95th percentile outpo<strong>in</strong>ts for<br />
lipoprote<strong>in</strong> triglyceride <strong>and</strong> cholesterol concentrations<br />
<strong>in</strong> late gestation that we have recently described.<br />
5<br />
Subjects<br />
Methods<br />
Twenty-three pregnant women with a physiologic<br />
plasma lipid <strong>in</strong>crease <strong>in</strong> pregnancy were recruited for<br />
this study from the classes of the Childbirth Education<br />
Association (CEA) <strong>in</strong> Seattle <strong>and</strong> K<strong>in</strong>g County.<br />
Six other pregnant women with supraphysiologic lipid<br />
<strong>in</strong>creases <strong>in</strong> pregnancy were referred or found<br />
through surveys. Two of these subjects, one hypertriglyceridemic<br />
(Subject DR), <strong>and</strong> one hypercholesterolemic<br />
(Subject AM), were identified <strong>in</strong> the orig<strong>in</strong>al<br />
CEA survey. All subjects gave <strong>in</strong>formed written consent.<br />
A physiologic <strong>in</strong>crease <strong>in</strong> plasma lipids <strong>in</strong> pregnancy<br />
was def<strong>in</strong>ed as a total plasma triglyceride <strong>and</strong><br />
cholesterol concentration less than the 95th percentile<br />
at 36 weeks of gestation (387 mg/dl for triglyceride<br />
<strong>and</strong> 318 mg/dl for cholesterol). 5 A supraphysiologic<br />
<strong>in</strong>crease <strong>in</strong> plasma lipids <strong>in</strong> pregnancy was<br />
def<strong>in</strong>ed as a total plasma triglyceride or cholesterol<br />
concentration at or above the 95th percentile at 36<br />
weeks of gestation. The pregnant subjects were<br />
compared with 23 nonpregnant subjects matched for<br />
age <strong>and</strong> Quetelet Index (body mass <strong>in</strong>dex calculated<br />
as weight/height 2 x 1000) with the 20-week postpartum<br />
body mass <strong>in</strong>dex of the study subjects used for<br />
match<strong>in</strong>g to controls. Control subjects were drawn<br />
from a r<strong>and</strong>om sample of female Pacific Northwest<br />
Bell Company employees whose characteristics<br />
were described previously. 8 " 8 The nonpregnant controls<br />
<strong>and</strong> 20-week postpartum subjects hav<strong>in</strong>g antepartum<br />
physiological <strong>in</strong>creases <strong>in</strong> blood lipids were<br />
closely matched for age, weight, height, <strong>and</strong> body<br />
mass <strong>in</strong>dex (Table 1). Women with supraphysiologic<br />
lipid <strong>in</strong>creases were generally heavier <strong>and</strong> had a<br />
higher Quetelet Index.<br />
Length of gestation was estimated from the first<br />
day of the last menstrual period. Pregnant subjects<br />
were studied with<strong>in</strong> 2 weeks of the antepartum target<br />
week <strong>and</strong> with<strong>in</strong> 1 week of the postpartum target<br />
week. All subjects were free-liv<strong>in</strong>g <strong>and</strong> consum<strong>in</strong>g<br />
their customary diets; there was no systematic attempt<br />
to restrict calories <strong>in</strong> these subjects. All fast<strong>in</strong>g<br />
glucose concentrations were normal <strong>in</strong> the pregnant<br />
subjects (mean 72.6 ± 1.6 mg/dl, range 60-87) <strong>and</strong><br />
<strong>in</strong> nonpregnant subjects (91.5 ± 7.6 mg/dl, range<br />
79-108). No medications except multivitam<strong>in</strong>s were<br />
taken dur<strong>in</strong>g pregnancy. All newborn <strong>in</strong>fants were<br />
healthy <strong>and</strong> of normal weight (mean 3581 g ± 87.6,<br />
range 2727-3949 g), except one who was anencephalic.<br />
The lipid <strong>and</strong> apoprote<strong>in</strong> measurements <strong>in</strong><br />
the mother of this <strong>in</strong>fant were typical. Of the women<br />
with physiological hyperlipidemia, 19 women breastfed<br />
postpartum <strong>and</strong> four did not. None took oral contraceptives<br />
dur<strong>in</strong>g the postpartum study period. One<br />
other woman (Subject EW) was studied before, as<br />
well as dur<strong>in</strong>g <strong>and</strong> after, pregnancy. Her results are<br />
considered separately. She was normoglycemic <strong>and</strong><br />
delivered a normal <strong>in</strong>fant weigh<strong>in</strong>g 3580 g. The lactational<br />
status of the women with supraphysiologic lipid<br />
<strong>in</strong>creases are noted <strong>in</strong> the tables or text. None used<br />
oral contraception postpartum.<br />
Table 1. Characteristics of Pregnant Subjects with <strong>Physiologic</strong> or <strong>Supraphysiologic</strong> Lipid<br />
<strong>Increases</strong> <strong>and</strong> Nonpregnant Normal Controls<br />
<strong>Physiologic</strong> <strong>in</strong>crease<br />
Antepartum week 34-38<br />
Postpartum week 6<br />
Postpartum week 20<br />
Nonpregnant controls<br />
<strong>Supraphysiologic</strong> <strong>in</strong>crease<br />
Triglyceride<br />
D.R.<br />
F.S.<br />
Y.F.<br />
C.B.<br />
Cholesterol<br />
M.R.<br />
N.C.<br />
Values are means ± SD.<br />
*Prepregnant body weight.<br />
No.<br />
23<br />
—<br />
—<br />
23<br />
Age<br />
(yrs)<br />
28.0 ±4.2<br />
—<br />
—<br />
27.8±4.2<br />
26<br />
32<br />
27<br />
27<br />
34<br />
30<br />
Weight<br />
(kg)<br />
70.6±7.1<br />
62.2±7.7<br />
60.6±8.7<br />
60.3 ±8.1<br />
64.5*<br />
84.5<br />
80.4<br />
69.6<br />
64.5<br />
55.2<br />
Height<br />
(cm)<br />
167.6 ±6.4<br />
—<br />
—<br />
166.5±6.0<br />
162.6<br />
172.7<br />
162.6<br />
165.0<br />
154.9<br />
165.1<br />
Downloaded from<br />
http://atvb.ahajournals.org/ by guest on June 29, 2013<br />
Body mass<br />
<strong>in</strong>dex<br />
(kg/cm 2 x<br />
1000)<br />
2.52 ±0.30<br />
2.22 + 0.22<br />
2.16±0.29<br />
2.17±0.23<br />
0.244*<br />
0.283<br />
0.304<br />
0.256<br />
0.269<br />
0.203
Blood Sampl<strong>in</strong>g<br />
PREGNANCY HYPERLIPIDEMIA AND PRELIPEMIA Montes et al. 409<br />
Blood samples <strong>in</strong> pregnant <strong>and</strong> postpartum women<br />
were obta<strong>in</strong>ed by a research nurse <strong>in</strong> each subject's<br />
home to m<strong>in</strong>imize the effects of stress on fuel<br />
<strong>and</strong> lipoprote<strong>in</strong> homeostasis. Nonpregnant subjects<br />
came to the Northwest Lipid Research Cl<strong>in</strong>ic for<br />
blood draw<strong>in</strong>g. All subjects had fasted for 12 to 14<br />
hours before the sampl<strong>in</strong>g. About 35 ml of venous<br />
blood were obta<strong>in</strong>ed from subjects who were sitt<strong>in</strong>g.<br />
The blood for lipid analysis conta<strong>in</strong>ed 1.5 mg EDTA<br />
per ml blood <strong>and</strong> was kept on ice until centrifuged <strong>in</strong><br />
the laboratory. The blood for glucose estimation was<br />
collected <strong>in</strong> tubes conta<strong>in</strong><strong>in</strong>g 2.5 mg sodium fluoride<br />
<strong>and</strong> 2.0 mg potassium oxalate per ml blood.<br />
Lipoprote<strong>in</strong> <strong>and</strong> Apoproteln Analyses<br />
Plasma samples were overla<strong>in</strong> with 0.9% sal<strong>in</strong>e<br />
<strong>and</strong> ultracentrifuged <strong>in</strong> a 40.3 rotor at 40,000 rpm at<br />
17° C for 18 hours. 9 The top 2 ml were analyzed as<br />
very low density lipoprote<strong>in</strong> (VLDL). The bottom fraction<br />
was brought to a measured 5 ml with sal<strong>in</strong>e <strong>and</strong><br />
analyzed as the d > 1.006 fraction. Another 3 ml of<br />
whole plasma was treated with hepar<strong>in</strong> <strong>and</strong> MnCLg<br />
to precipitate VLDL <strong>and</strong> low density lipoprote<strong>in</strong><br />
(LDL), allow<strong>in</strong>g measurement of high density lipoprote<strong>in</strong><br />
(HDL) lipids <strong>in</strong> the supernatant. 9 ' 10 The apo B<br />
content of the supernatant fraction never exceeded 2<br />
mg/dl by immunoassay. LDL lipid concentrations<br />
were determ<strong>in</strong>ed as the difference between the d <<br />
1.006 <strong>in</strong>franatant <strong>and</strong> HDL. Triglyceride <strong>and</strong> cholesterol<br />
were measured us<strong>in</strong>g the AutoAnalyzer II<br />
method. 9<br />
Apolipoprote<strong>in</strong> B (apo B) was measured <strong>in</strong> total<br />
plasma <strong>and</strong> VLDL by a double antibody radioimmu-<br />
noassay as previously described. 11 LDL apo B was<br />
calculated as the difference between total plasma<br />
<strong>and</strong> VLDL apo B. Apolipoprote<strong>in</strong> A-l was measured<br />
on whole plasma by a radial immunodiffusion method<br />
after tetramethylurea delipidation. 12<br />
The ratios of triglyceride/cholesterol <strong>and</strong> lipid/apoprote<strong>in</strong><br />
<strong>in</strong> each lipoprote<strong>in</strong> fraction are presented as<br />
<strong>in</strong>dices of lipoprote<strong>in</strong> composition.<br />
Statistical Analyses<br />
The mean, st<strong>and</strong>ard deviation, <strong>and</strong> median described<br />
lipoprote<strong>in</strong> lipids, apoprote<strong>in</strong>s <strong>and</strong> ratios for<br />
the nonpregnant controls <strong>and</strong> the antepartum <strong>and</strong><br />
postpartum subjects. Nonparametric statistical<br />
methods were used for significance test<strong>in</strong>g because<br />
of the small sample sizes. Wilcoxon's matched pairs<br />
test 13 was performed to determ<strong>in</strong>e if significant differences<br />
existed between antepartum <strong>and</strong> postpartum<br />
measurements <strong>and</strong> between 6- <strong>and</strong> 20-week postpartum<br />
values. The Wilcoxon rank sum test 13 was<br />
used to detect differences between controls <strong>and</strong> antepartum,<br />
6-week, <strong>and</strong> 20-week postpartum subjects.<br />
Mean values <strong>and</strong> 95% confidence <strong>in</strong>tervals<br />
were used to graphically illustrate antepartum-topostpartum<br />
changes.<br />
Results<br />
<strong>Physiologic</strong> Hyperllpldemla In Pregnancy<br />
Table 2 presents the antepartum-postpartum lipoprote<strong>in</strong><br />
observations <strong>in</strong> subjects with physiologic<br />
hyperlipidemia <strong>in</strong> pregnancy <strong>and</strong> matched nonpregnant<br />
controls. Selected lipoprote<strong>in</strong> lipid <strong>and</strong> apoprote<strong>in</strong><br />
changes are illustrated <strong>in</strong> Figure 1. Ratios of<br />
Table 2. Plasma Lipoprote<strong>in</strong> Lipid <strong>and</strong> Apoproteln Concentrations (mg/dl) <strong>in</strong> 23 Women In Late<br />
Pregnancy <strong>and</strong> Postpartum <strong>and</strong> <strong>in</strong> 23 Age- <strong>and</strong> Body-Mass-Matched Nonpregnant Controls<br />
Total<br />
Triglyceride<br />
Cholesterol<br />
Pregnant<br />
Weeks 34-38<br />
Mean±SD Median Mean<br />
222 ±60<br />
251 ±32<br />
223*<br />
244*<br />
VLDL<br />
Triglyceride 107 ±41 100*<br />
Cholesterol 22 ± 9 20*<br />
ApoB 20±11 23*<br />
LDL<br />
Triglyceride<br />
Cholesterol<br />
ApoB<br />
HDL<br />
Triglyceride<br />
Cholesterol<br />
ApoA-1<br />
72 ±21<br />
161 ±39<br />
84±23<br />
29 ±9<br />
64 ± 9<br />
164+16<br />
70<br />
151*<br />
81*<br />
26*<br />
65*<br />
167*<br />
Week 6 Week 20<br />
±SD<br />
71 ±23<br />
205 + 23<br />
Postpartum<br />
Median Mean ± so<br />
66t<br />
204*t<br />
29±18 23t<br />
7±4 6*f<br />
4±3 4t<br />
27 + 10<br />
124±21<br />
104±17<br />
8±3<br />
64±12<br />
127±22<br />
26*t<br />
127*t<br />
103*f<br />
9*t<br />
62*<br />
130t<br />
'Significantly different from controls at p s 0.05.<br />
tSignificantly different from antepartum at p < 0.05.<br />
^Significantly different from 6 week postpartum at p < 0.05.<br />
66±18<br />
190±28<br />
Median<br />
62t<br />
187*t*<br />
28±16 21t<br />
6±5 5't<br />
4±2 4t<br />
23±7 21*t<br />
120 ±24 120't<br />
88 ±16 90*tt<br />
8±4<br />
56±11<br />
132±16<br />
10t<br />
131f<br />
Downloaded from<br />
http://atvb.ahajournals.org/ by guest on June 29, 2013<br />
Nonpregnant controls<br />
Mean±sD<br />
59±19<br />
171+26<br />
33±14<br />
11+6<br />
7 + 6<br />
14±10<br />
104±23<br />
61 ±10<br />
12±6<br />
56±12<br />
128±23<br />
Median<br />
58<br />
165<br />
31<br />
10<br />
6<br />
13<br />
103<br />
62<br />
11<br />
53<br />
124
410 ARTERIOSCLEROSIS VOL 4, No 4, JULY/AUGUST 1984<br />
50-<br />
LDL:<br />
150-<br />
2* 100 H<br />
HDL:<br />
150-<br />
100-<br />
50-<br />
Weeks. 36<br />
PREGNANCY HYPERLIPIDEMIA AND PRELIPEMIA Montes et al. 411<br />
Table 3. LIpoprote<strong>in</strong> Lipid <strong>and</strong> Apoproteln Ratios In 23 Women <strong>in</strong> Late Pregnancy <strong>and</strong> Postpartum <strong>and</strong> In 23<br />
Age- <strong>and</strong> Body-Mass-Matched Nonpregnant Controls<br />
VLDL<br />
TG/chol<br />
TG/apo B<br />
Chol/apo B<br />
LDL<br />
TG/chol<br />
TG/apo B<br />
Chol/apo B<br />
HDL<br />
TG/chol<br />
TG/apo A-1<br />
Chol/apo A-1<br />
Pregnant<br />
Weeks 34-38<br />
Mean±SD Median Mean<br />
5.10±1.10 5.00*<br />
7.79 ±5.07 5.21<br />
1.57 ±0.98 0.99<br />
0.46±0.10<br />
0.91 ±0.30<br />
2.02 + 0.65<br />
0.44*<br />
0.87*<br />
1.93<br />
0.46 ±0.15 0.50*<br />
0.18±0.05 0.16*<br />
0.39 ±0.07 0.40*<br />
Week 6 Week 20<br />
±SD<br />
4.88 ±2.40 4.00*<br />
9.30±9.08 7.00<br />
2.31+3.07 1.60<br />
0.23 ±0.08<br />
0.26 + 0.08<br />
1.21 ±0.25<br />
0.14±0.06<br />
0.07 ±0.03<br />
0.51 ±0.11<br />
Postpartum<br />
Median Mean±sD<br />
0.22*t<br />
0.25f<br />
1.14*t<br />
0.13*t<br />
0.07t<br />
0.48*t<br />
'Significantly different from controls at p s 0.05.<br />
tSignificantly different from antepartum at p == 0.05.<br />
^Significantly different from 6 weeks postpartum at p ^ 0.05.<br />
80-<br />
60-<br />
I6O-<br />
80-<br />
mg/dl<br />
240-<br />
I6O<br />
80-<br />
O- 1<br />
Glucose<br />
Triglycerkje<br />
Cholesterol<br />
8 16 24<br />
Pregnancy<br />
6.14±3.76<br />
7.56 ±4.01<br />
1.50 ±1.02<br />
0.20 ±0.07<br />
0.26 ±0.08<br />
1.38 ±0.29<br />
0.15 ±0.08<br />
0.07 + 0.03<br />
0.42 ±0.08<br />
32 40<br />
Weeks<br />
Median<br />
5.67*<br />
6.18<br />
1.15<br />
0.20*t<br />
0.25f<br />
1.43*t<br />
0.16*t<br />
0.07*t<br />
-VLDL<br />
Nonpregnant controls<br />
Mean±sD<br />
3.69 ±3.48<br />
10.88± 14.86<br />
3.06 ±3.32<br />
0.14 + 0.08<br />
0.23±0.17<br />
1.72 ±0.28<br />
0.21 ±0.09<br />
0.09 ±0.04<br />
0.44 + 0.06<br />
LDL<br />
6 20<br />
Posfpartum<br />
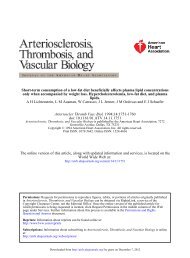
Figure 2. Plasma glucose, triglyceride, <strong>and</strong> cholesterol <strong>and</strong> lipoprote<strong>in</strong> cholesterol<br />
concentrations <strong>in</strong> subject EW before, dur<strong>in</strong>g, <strong>and</strong> after pregnancy. Glucose decl<strong>in</strong>ed<br />
while all lipids <strong>in</strong>creased throughout pregnancy. Postpartum, triglyceride <strong>and</strong> VLDL<br />
cholesterol fell to slightly below prepregnancy levels by 6 weeks of gestation <strong>and</strong> HDL<br />
cholesterol fell to normal by 20 weeks. LDL cholesterol decl<strong>in</strong>ed more slowly <strong>and</strong><br />
rema<strong>in</strong>ed above prepregnancy levels at 20 weeks postpartum.<br />
Downloaded from<br />
http://atvb.ahajournals.org/ by guest on June 29, 2013<br />
Median<br />
2.99<br />
4.11<br />
1.50<br />
0.12<br />
0.22<br />
1.74<br />
0.20<br />
0.09<br />
0.44
412 ARTERIOSCLEROSIS VOL 4, No 4, JULY/AUGUST 1984<br />
Table 4. Hypertrlglycerldemla In Pregnancy: Subject D.R.<br />
Pregnant<br />
Week 36<br />
Week 6<br />
Whole plasma (mg/dl)<br />
Triglyceride<br />
Cholesterol<br />
VLDL (mg/dl)<br />
Triglyceride<br />
Cholesterol<br />
Apo B<br />
LDL (mg/dl)<br />
Triglyceride<br />
Cholesterol<br />
Apo B<br />
HDL (mg/dl)<br />
Triglyceride<br />
Cholesterol<br />
Apo A-1<br />
600<br />
329<br />
382<br />
79<br />
44<br />
164<br />
240<br />
181<br />
10<br />
14<br />
158<br />
(387)*<br />
(318)<br />
(246)<br />
(47)<br />
(113)<br />
(218)<br />
121<br />
(21)<br />
(42)<br />
95<br />
211<br />
169<br />
131<br />
23<br />
9<br />
34<br />
114<br />
99<br />
7<br />
12<br />
95<br />
(157)*<br />
(265)<br />
(122)<br />
(29)<br />
(36)<br />
(177)<br />
(4)<br />
(44)<br />
Postpartum<br />
Week 20<br />
102<br />
163<br />
69<br />
15<br />
7<br />
24<br />
109<br />
6<br />
36<br />
116<br />
(127)*<br />
(225)<br />
(83)<br />
(28)<br />
(35)<br />
(157)<br />
(5)<br />
(35)<br />
Week 40<br />
115<br />
154<br />
71<br />
17<br />
25<br />
97<br />
15<br />
40<br />
(127)*<br />
(225)<br />
(83)<br />
(28)<br />
(35)<br />
(157)<br />
D.R.'s <strong>in</strong>fant's birth weight was 3239 g. D.R. elected not to breast feed postpartum or use oral<br />
contraceptives. See text for family study lipids.<br />
'Denotes 95th percentiles for total, VLDL, <strong>and</strong> LDL lipids <strong>and</strong> 5th percentile for HDL lipids. Values for<br />
36 weeks of gestation <strong>and</strong> 6 weeks postpartum are based on a study of 553 pregnant women (see<br />
reference 5); values are from reference 6 for 20- to 29-year-old nonpregnant, nonhormone-tak<strong>in</strong>g subjects<br />
(Weeks 20 <strong>and</strong> 40).<br />
Table 5. Summary of Endogenous Hypertrlglycerldemic Subjects Studied In Pregnancy<br />
Pre-<br />
Pregnant<br />
Postpartum<br />
pregnant Week 36 Week 6 20 40 100<br />
Total triglyceride (mg/dl)<br />
(95th percentile)<br />
D.R.<br />
F.S.<br />
Y.F.<br />
C.B.<br />
Total cholesterol (mg/dl)<br />
(95th percentile)<br />
D.R.<br />
F.S.<br />
Y.F.<br />
C.B.<br />
LDL cholesterol (mg/dl)<br />
(95th percentile)<br />
D.R.<br />
F.S.<br />
Y.F.<br />
C.B.<br />
HDL cholesterol (mg/dl)<br />
(95th percentile)<br />
D.R.<br />
F.S.<br />
Y.F.<br />
C.B.<br />
(127)*<br />
—<br />
—<br />
—<br />
116<br />
(225)<br />
—<br />
—<br />
—<br />
223<br />
(157)<br />
—<br />
—<br />
160<br />
(35)<br />
—<br />
—<br />
40<br />
(387)t<br />
600<br />
434<br />
716<br />
1195<br />
(318)<br />
329<br />
184<br />
257<br />
274<br />
(218)<br />
240<br />
70<br />
60<br />
61<br />
(42)<br />
14<br />
40<br />
43<br />
38<br />
(157)t<br />
211<br />
179<br />
221<br />
392<br />
(265)<br />
169<br />
212<br />
267<br />
260<br />
(177)<br />
114<br />
152<br />
187<br />
163<br />
(44)<br />
12<br />
34<br />
36<br />
36<br />
(127)*<br />
102<br />
124<br />
151<br />
—<br />
(225)<br />
163<br />
169<br />
205<br />
—<br />
(157)<br />
109<br />
124<br />
124<br />
—<br />
(35)<br />
36<br />
29<br />
32<br />
—<br />
(127)*<br />
115<br />
—<br />
—<br />
570<br />
(225)<br />
154<br />
—<br />
—<br />
232<br />
(157)<br />
97<br />
—<br />
—<br />
—<br />
*Percentiles from a population of nonpregnant subjects (see reference 6).<br />
tPercentiles from a population study of pregnant <strong>and</strong> postpartum subjects (see reference 5).<br />
Downloaded from<br />
http://atvb.ahajournals.org/ by guest on June 29, 2013<br />
(35)<br />
40<br />
—<br />
—<br />
34<br />
(5)<br />
(35)<br />
(127)*<br />
—<br />
—<br />
—<br />
173<br />
(225)<br />
—<br />
—<br />
—<br />
213<br />
(157)<br />
—<br />
—<br />
—<br />
139<br />
(35)<br />
—<br />
—<br />
—<br />
39
PREGNANCY HYPERLIPIDEMIA AND PRELIPEMIA Montes et al. 413<br />
/ /<br />
£• £• 6<br />
20 40 60<br />
Weeks Postpartum<br />
Figure 3. Plasma total triglyceride <strong>and</strong> LDL <strong>and</strong> HDL cholesterol concentrations<br />
antepartum, at 36 weeks of gestation, <strong>and</strong> at various times postpartum <strong>in</strong> four hypertriglyceridemic<br />
subjects <strong>in</strong> pregnancy compared with the 95th or 5th percentiles of a<br />
r<strong>and</strong>om population of pregnant women or nonpregnant women aged 20 to 29 years.<br />
Total triglyceride for subject YF (aged 33) is above the 95th percentile for women aged<br />
20-29 at 20 weeks postpartum, but below the 95th percentile for women aged 30-39.<br />
<strong>Supraphysiologic</strong> Hyperlpidemia <strong>in</strong> Pregnancy<br />
The results are considered by the <strong>in</strong>dividual subject<br />
<strong>in</strong> the text <strong>and</strong> are summarized <strong>in</strong> Tables 4 to 6<br />
<strong>and</strong> Figure 3. Subject DR was studied <strong>in</strong> detail (Table<br />
4 <strong>and</strong> Figure 3). She was markedly hypertriglyceridemic<br />
<strong>and</strong> slightly hypercholesterolemic <strong>in</strong> late gestation<br />
as compared to 95th percentile reference values.<br />
5 The VLDL triglyceride level of 382 mg/dl was<br />
well above the 95th percentile <strong>in</strong> pregnancy (246 mg/<br />
dl). The LDL triglyceride <strong>and</strong> cholesterol concentrations<br />
both exceeded the 95th percentile at 36 weeks<br />
of gestation, but the relative amounts of her triglyceride,<br />
cholesterol, <strong>and</strong> apo B <strong>in</strong> LDL rema<strong>in</strong>ed approximately<br />
the same as <strong>in</strong> the 23 normal subjects (Table<br />
2). Her HDL triglyceride <strong>and</strong> cholesterol concentrations<br />
were markedly reduced <strong>in</strong> pregnancy, while the<br />
apo A-l concentrations rema<strong>in</strong>ed at a level typical for<br />
pregnancy (158 mg/dl).<br />
At 6 weeks postpartum, DR's plasma triglyceride<br />
concentrations rema<strong>in</strong>ed above the 95th percentile,<br />
but at 20 <strong>and</strong> 40 weeks postpartum they fell with<strong>in</strong><br />
the 95th percentile of triglyceride for nonpregnant,<br />
nonhormone-us<strong>in</strong>g subjects. 6 A similar slow postpartum<br />
decl<strong>in</strong>e was seen for VLDL triglyceride. LDL tri-<br />
100<br />
glycerides had dropped more abruptly by 6 weeks<br />
postpartum, while HDL triglyceride decl<strong>in</strong>ed slowly.<br />
LDL cholesterol showed a cont<strong>in</strong>u<strong>in</strong>g decl<strong>in</strong>e<br />
through 40 weeks postpartum but was with<strong>in</strong> the<br />
95th percentile by 6 weeks postpartum. HDL cholesterol<br />
was still low at 6 weeks postpartum, rose by 20<br />
weeks postpartum, but even at 40 weeks postpartum<br />
was only marg<strong>in</strong>ally above the 5th percentile for HDL<br />
cholesterol <strong>in</strong> nonpregnant women aged 20-29. In<br />
contrast, apo A-l concentrations at 6 <strong>and</strong> 20 weeks<br />
postpartum were only slightly below the mean for<br />
nonpregnant, nonhormone-treated normal subjects<br />
(125 mg/dl). 12<br />
Two years later, subject DR was observed <strong>in</strong> a<br />
second pregnancy at 36 weeks of gestation. Total<br />
plasma triglyceride was 400 mg/dl (>95th percentile),<br />
LDL cholesterol was 167 mg/dl (
414 ARTERIOSCLEROSIS VOL 4, No 4, JULY/AUGUST 1984<br />
Table 6. Hypercholesterolemla In Pregnancy:<br />
Subject A.M.<br />
Whole plasma<br />
Triglyceride<br />
Cholesterol<br />
VLDL (mg/dl)<br />
Triglyceride<br />
Cholesterol<br />
Apo B<br />
LDL (mg/dl)<br />
Triglyceride<br />
Cholesterol<br />
Apo B<br />
HDL (mg/dl)<br />
Triglyceride<br />
Cholesterol<br />
Apo A-1<br />
Pregnant<br />
Week 36<br />
(mg/dl)<br />
226 (387)<br />
326 (318)<br />
87 (246)<br />
15 (47)<br />
20<br />
98 (113)<br />
230 (218)<br />
116<br />
23 (21)<br />
60 (42)<br />
164<br />
Postpartum<br />
Week 6 Week 20<br />
118 (157)<br />
250 (265)<br />
40 (122)<br />
9 (29)<br />
11<br />
50 (36)<br />
167 (177)<br />
184<br />
13 (4)<br />
59 (44)<br />
150<br />
105 (160)<br />
254 (240)<br />
20 (112)<br />
4 (28)<br />
4<br />
68 (28)<br />
181 (159)<br />
103<br />
11 (4)<br />
52 (33)<br />
150<br />
A.M.'s <strong>in</strong>fant's birth weight was 2789 g. A.M. breast fed<br />
for 8 weeks postpartum.<br />
Parentheses denote 95th percentiles for total, VLDL,<br />
<strong>and</strong> LDL lipids <strong>and</strong> 5th percentile for HDL lipids. Values for<br />
36 weeks of gestation <strong>and</strong> 6 weeks postpartum are based<br />
on a study of 553 pregnant women (see reference 5);<br />
values for age 30-39 nonpregnant, nonhormone-tak<strong>in</strong>g<br />
subjects (Week 20) are from reference 6.<br />
242 (>90th age-specific percentile), a total-cholesterol<br />
of 257 (>75th percentile), an LDL cholesterol of<br />
181 (~90th percenile), <strong>and</strong> an HDL cholesterol of 37<br />
(~15th percentile). The mother's lipoprote<strong>in</strong>s were<br />
close to the median values for her age <strong>and</strong> sex: total<br />
triglyceride, 149; total cholesterol, 227; LDL cholesterol,<br />
175; while her HDL cholesterol, 72 mg, was<br />
near the 75th percentile. Thus, there is evidence for<br />
elevated total triglyceride <strong>and</strong> LDL cholesterol <strong>in</strong> a<br />
first degree relative of DR.<br />
Three other subjects with supraphysiologic triglyceride<br />
<strong>in</strong>creases <strong>in</strong> pregnancy are compared to DR <strong>in</strong><br />
Table 5 <strong>and</strong> are also illustrated <strong>in</strong> Figure 3. One of<br />
these women, subject CB, was the mother of two<br />
hypertriglyceridemic children with fast<strong>in</strong>g chylomicronemia<br />
<strong>and</strong> plasma triglyceride levels of 6460 <strong>and</strong><br />
796 mg/dl at ages 3 <strong>and</strong> 1, respectively, on an unrestricted<br />
diet. CB's parents had triglycerides at the<br />
75th <strong>and</strong> 90th percentiles <strong>and</strong> cholesterol at the 75th<br />
percentile. 68 CB therefore appears to be an obligate<br />
heterozygote for the Type I phenotype. YF's brother<br />
(aged 29) had total <strong>and</strong> LDL cholesterol concentrations<br />
(237 <strong>and</strong> 163 mg/dl, respectively) at or above<br />
the age- <strong>and</strong> sex-specific 95th percentiles (222 <strong>and</strong><br />
165 mg/dl) <strong>and</strong> a total triglyceride concentration (135<br />
mg/dl) >90th percentile. YF's father had average<br />
lipoprote<strong>in</strong> lipid concentrations. Thus, there is an association<br />
of hyperlipidemia <strong>in</strong> a first degree relative<br />
of YF. The relatives of FS were not available for<br />
study.<br />
All four subjects were below the 95th percentile<br />
values for total plasma triglycerides either before<br />
Downloaded from<br />
http://atvb.ahajournals.org/ by guest on June 29, 2013<br />
pregnancy or 20 weeks postpartum, but were markedly<br />
above the 95th percentile <strong>in</strong> late gestation. All<br />
subjects showed a delay <strong>in</strong> the postpartum decl<strong>in</strong>e of<br />
total triglyceride concentrations compared with normal<br />
subjects, <strong>in</strong> that at 6 weeks postpartum, total<br />
triglyceride concentrations were consistently above<br />
the 95th percentile (Table 5 <strong>and</strong> Figure 3). Similar<br />
trends were observed <strong>in</strong> VLDL triglyceride <strong>and</strong> cholesterol<br />
(data not shown). Disparate responses were<br />
seen among the four subjects with respect to total<br />
<strong>and</strong> LDL cholesterol ante- <strong>and</strong> postpartum. DR was<br />
the only subject show<strong>in</strong>g a comb<strong>in</strong>ed elevation of<br />
triglyceride <strong>and</strong> cholesterol <strong>in</strong> pregnancy. All others<br />
had abnormal <strong>in</strong>creases only <strong>in</strong> total <strong>and</strong> VLDL triglyceride.<br />
Another dist<strong>in</strong>ction was the LDL cholesterol<br />
fall at 6 weeks postpartum <strong>in</strong> DR, but a rise <strong>in</strong> the<br />
other three. The 20-week postpartum or prepregnancy<br />
LDL cholesterol concentrations <strong>in</strong> these three<br />
subjects were also higher than the pregnancy levels.<br />
HDL cholesterol concentrations were not as low <strong>in</strong><br />
subjects FS, YF, <strong>and</strong> CB as <strong>in</strong> subject DR, but were<br />
near or below the 5th percentiles both ante- <strong>and</strong><br />
postpartum.<br />
Hypercholesterolemic subject AM is presented <strong>in</strong><br />
Table 6 <strong>and</strong> <strong>in</strong> Figure 3. She was not on a cholesterol-restricted<br />
diet at the time of the study. Total plasma<br />
cholesterol concentrations were similar at 6 <strong>and</strong><br />
20 weeks postpartum, but were near or above the<br />
95th percentile value. VLDL lipids <strong>and</strong> apo B were<br />
consistently normal (compare the apo B results with<br />
those <strong>in</strong> Table 2). The LDL cholesterol concentration<br />
was above the 95th percentile at 36 weeks of gestation,<br />
5 fell postpartum to slightly below the 95th percentile<br />
at 6 weeks, but exceeded the 95th percentile<br />
at 20 weeks. 6 Compared with 6 <strong>and</strong> 20 weeks postpartum,<br />
the LDL cholesterol rise due to pregnancy<br />
was 49 to 63 mg/dl. The apo B concentration was<br />
about 40 mg/dl above the average at 36 weeks of<br />
gestation <strong>and</strong> 20 weeks postpartum, but <strong>in</strong>creased to<br />
80 mg/dl above the average at 6 weeks postpartum,<br />
an exaggeration of the pattern observed <strong>in</strong> normal<br />
subjects at 6 weeks postpartum (Table 2). HDL lipids<br />
were fairly typical <strong>in</strong> this patient; however, apo A-l did<br />
not fall postpartum as much as expected.<br />
A familial heterozygous hypercholesterolemic<br />
woman with tendonous xanthomas (subject NC) was<br />
studied at 37 weeks of gestation <strong>and</strong> 6 <strong>and</strong> 20 weeks<br />
postpartum. The patient was on a cholesterol-restricted<br />
<strong>and</strong> polyunsaturate-supplemented diet<br />
throughout. Total cholesterol was 614 mg/dl <strong>and</strong> total<br />
triglyceride, 232 mg/dl at 37 weeks of gestation.<br />
Postpartum, 6- <strong>and</strong> 20-week total cholesterol concentrations<br />
were 554 mg/dl <strong>and</strong> 530 mg/dl with cholesterol<br />
concentrations <strong>in</strong> VLDL of 20 mg/dl <strong>and</strong> 24<br />
mg/dl; LDL, of 484 mg/dl <strong>and</strong> 444 mg/dl; <strong>and</strong> HDL, of<br />
60 mg/dl <strong>and</strong> 62 mg/dl. In NC the total cholesterol<br />
rise <strong>in</strong> pregnancy (compar<strong>in</strong>g 36 weeks of gestation<br />
<strong>and</strong> 20 weeks postpartum) was 84 mg/dl, only slightly<br />
higher than the total cholesterol <strong>in</strong>crement observed<br />
<strong>in</strong> 23 normal women over the same <strong>in</strong>terval<br />
(61 mg/dl). The conclusion from hypecholesterole
PREGNANCY HYPERLIPIDEMIA AND PRELIPEMIA Montes et al. 415<br />
mic subjects AM <strong>and</strong> NC is that plasma cholesterol <strong>in</strong><br />
hypercholesterolemic subjects is not disproportionately<br />
exaggerated <strong>in</strong> pregnancy <strong>in</strong> contrast to plasma<br />
triglyceride <strong>in</strong> hypertriglyceridemics.<br />
Discussion<br />
Women with physiologic or supraphysiologic <strong>in</strong>creases<br />
<strong>in</strong> plasma triglyceride or cholesterol <strong>in</strong> pregnancy<br />
were studied at 34 to 38 weeks of gestation<br />
<strong>and</strong> at 6 <strong>and</strong> 20 weeks or longer postpartum to answer<br />
the follow<strong>in</strong>g questions: How rapidly do the<br />
changes <strong>in</strong> plasma lipoprote<strong>in</strong>s return to normal<br />
postpartum <strong>in</strong> subjects who have a physiologic lipid<br />
<strong>in</strong>crease antepartum? Do subjects with supraphysiologic<br />
<strong>in</strong>creases antepartum return to normal postpartum<br />
<strong>in</strong> the same manner <strong>and</strong> do they return to normal<br />
at all? Are there identify<strong>in</strong>g characteristics <strong>in</strong> lipoprote<strong>in</strong><br />
concentrations or family history that would suggest<br />
that the supraphysiologic lipid rise <strong>in</strong> pregnancy<br />
is a pathophysiologic process <strong>in</strong>dicative of a subcl<strong>in</strong>ical<br />
or prelipemic trait that may eventually progress to<br />
overt hyperlipidemia?<br />
In subjects with a physiologic triglyceride rise <strong>in</strong><br />
pregnancy, plasma total triglyceride <strong>and</strong> all VLDL<br />
constituents reached a basel<strong>in</strong>e level by 6 weeks<br />
postpartum essentially identical to nonpregnant<br />
con In subjects with a physiologic triglyceride rise<br />
<strong>in</strong> pregnancy, plasma total triglyceride <strong>and</strong> all VLDL<br />
constituents reached a basel<strong>in</strong>e level by 6 weeks<br />
postpartum essentially identical to nonpregnant control<br />
subjects. All subjects with a supraphysiological<br />
triglyceride rise <strong>in</strong> pregnancy had normal total plasma<br />
triglyceride concentrations (
416 ARTERIOSCLEROSIS VOL 4, No 4, JULY/AUGUST 1984<br />
A f<strong>in</strong>al argument that a supraphysiologic rise <strong>in</strong><br />
plasma triglyceride antepartum is a pathophysiologic<br />
process signify<strong>in</strong>g an underly<strong>in</strong>g prelipemic trait is<br />
based on the fact that all three subjects for whom<br />
relatives were available show evidence of hyperlipidemia<br />
among family members. The difference<br />
among the subjects' responses to pregnancy, as well<br />
as the available <strong>in</strong>formation among relatives, suggests<br />
that the designation of prelipemia could represent<br />
several dist<strong>in</strong>ct <strong>and</strong> possibly genetic underly<strong>in</strong>g<br />
disorders of lipoprote<strong>in</strong> metabolism. Further <strong>in</strong>vestigations<br />
of larger numbers of prelipemic women with<br />
<strong>in</strong>-depth family studies are necessary to resolve this<br />
question. In addition, long-term follow-up will be necessary<br />
to verify the hypothesis that the hyperlipidemic<br />
stress of pregnancy can unmask a prelipemic<br />
trait. Nonetheless, it is noteworthy that subject CB<br />
has rema<strong>in</strong>ed hyperlipidemic for almost 2 years<br />
s<strong>in</strong>ce delivery, her only normal value hav<strong>in</strong>g been<br />
obta<strong>in</strong>ed before the pregnancy we observed.<br />
While the postpartum observations made at specific<br />
times <strong>and</strong> the dist<strong>in</strong>ctions between subjects with<br />
physiologic <strong>and</strong> supraphysiologic lipid <strong>in</strong>creases <strong>in</strong><br />
pregnancy are entirely new, our antepartum observations<br />
confirm several previously described features<br />
of hyperlipidemia <strong>in</strong> pregnancy. These <strong>in</strong>clude<br />
an <strong>in</strong>crease <strong>in</strong> total <strong>and</strong> VLDL apo B, 24 little or no<br />
change <strong>in</strong> VLDL composition, 2 2425 an <strong>in</strong>crease <strong>in</strong><br />
triglyceride content of LDL <strong>and</strong> HDL, 22425 <strong>and</strong> an<br />
<strong>in</strong>crease <strong>in</strong> apo A-l. 26 Thus, conclusions drawn from<br />
this paper can be considered to be generally representative<br />
of the body of <strong>in</strong>formation on hyperlipidemia<br />
<strong>in</strong> pregnancy.<br />
The possibility that the hyperlipidemia of pregnancy<br />
might confer added arteriosclerosis risk has<br />
recently been raised. 2728 While it is true that an <strong>in</strong>crease<br />
<strong>in</strong> LDL cholesterol could enhance arteriosclerosis,<br />
usually this change is associated with an apo<br />
B-rich 29 <strong>and</strong> triglyceride-poor LDL, 30 which is the opposite<br />
of that seen <strong>in</strong> pregnancy. In addition, HDL<br />
cholesterol <strong>and</strong> apo A-l concentrations were <strong>in</strong>creased,<br />
which may facilitate cholesterol removal<br />
from tissues. In light of these results, it is perhaps not<br />
surpris<strong>in</strong>g that the epidemiologic evidence 31 that<br />
arteriosclerosis is more common <strong>in</strong> multiparous<br />
women is <strong>in</strong>conclusive. It is more likely that the observed<br />
lipoprote<strong>in</strong> changes serve a physiological<br />
purpose to support growth of maternal <strong>and</strong> fetal tissues<br />
<strong>and</strong> production of large quantities of steroid<br />
hormones. 5 ' 16 The extent to which the postpartum<br />
lipoprote<strong>in</strong> changes are atherogenic is deserv<strong>in</strong>g of<br />
further study.<br />
In summary, evidence is presented to support the<br />
hypothesis that the hyperlipidemic stress of pregnancy<br />
can unmask a latent hypertriglyceridemia, by<br />
us<strong>in</strong>g as a basis for recognition a triglyceride rise <strong>in</strong><br />
pregnancy exceed<strong>in</strong>g the 95th percentile. Women<br />
with such a supraphysiologic triglyceride rise antepartum<br />
may return to normal levels postpartum more<br />
slowly than normal, have LDL lipids that change <strong>in</strong> an<br />
atypical manner antepartum <strong>and</strong> postpartum, have<br />
Downloaded from<br />
http://atvb.ahajournals.org/ by guest on June 29, 2013<br />
HDL cholesterol concentrations that are persistently<br />
low antepartum <strong>and</strong> postpartum, <strong>and</strong> have hyperlipidemic<br />
family members. In contrast, hypercholesterolemia<br />
is not greatly exaggerated <strong>in</strong> pregnancy. Longterm<br />
follow-up studies of women with genetically<br />
well-characterized disorders of lipoprote<strong>in</strong> metabolism<br />
are required to determ<strong>in</strong>e if an abnormal lipoprote<strong>in</strong><br />
response <strong>in</strong> pregnancy can identify prelipemic<br />
subjects <strong>and</strong> dist<strong>in</strong>guish among the major disorders<br />
of lipoprote<strong>in</strong> metabolism. Identification of prelipemia<br />
will provide an opportunity to study prospectively<br />
the natural progression, potential for atherosclerosis,<br />
<strong>and</strong> possible treatment of hyperlipidemia from<br />
early adulthood.<br />
Acknowledgments<br />
The authors express their thanks to the staff of the Northwest<br />
Liptd Research Cl<strong>in</strong>ic Core Laboratory who performed analyses;<br />
to Susan Irv<strong>in</strong>e who carefully obta<strong>in</strong>ed the samples; to the gracious<br />
women of the Childbirth Education Association who volunteered<br />
for participation <strong>in</strong> the study; <strong>and</strong> to Donna Gola <strong>and</strong> Lori<br />
Lebon for excellent secretarial assistance.<br />
References<br />
1. O'Sulllvan JB, Mahan CM. Criteria for the oral glucose tolerance<br />
test <strong>in</strong> pregnancy. Diabetes 1964;13:278-285<br />
2. Knopp RH, Warth MR, Carroll CJ. Lipid metabolism <strong>in</strong> pregnancy.<br />
I. Changes <strong>in</strong> lipoprote<strong>in</strong> triglyceride <strong>and</strong> cholesterol <strong>in</strong><br />
normal pregnancy <strong>and</strong> the effects of diabetes mellitus. J Reprod<br />
Med 1973;10:95-101<br />
3. D<strong>and</strong>row RV, O'Sulllvan JB. Obstetric hazards of gestational<br />
diabetes. Am J Obstet Gynecol 1966;96:1144-1147<br />
4. O'Sulllvan JB. Gestational diabetes: Unsuspected, a symptomatic<br />
diabetes <strong>in</strong> pregnancy. N Engl J Med 1961;264:<br />
1082-1085<br />
5. Knopp RH, Bergelln RO, Wahl PW, Walden CE, Chapman<br />
M, Irv<strong>in</strong>e S. Population-based lipoprote<strong>in</strong> lipid reference values<br />
for pregnant women compared to nonpregnant women<br />
classified by sex hormone use. Am J Obstet Gynecol<br />
1982;143:626-637<br />
6. Wahl PW, Walden CE, Albere JJ, et al. Distribution of lipoprote<strong>in</strong><br />
triglyceride <strong>and</strong> lipoprote<strong>in</strong> cholesterol <strong>in</strong> an adult population<br />
by age, sex, <strong>and</strong> hormone use: The Pacific Northwest<br />
Bell Telephone Company Health Survey. Atherosclerosis<br />
1981;39:111-124<br />
7. Knopp RH, Warnlck GR, Walden CE, el al. Relationship of<br />
gender, sex hormone use, <strong>and</strong> age with lipoprote<strong>in</strong> cholesterol/triglyceride<br />
ratios <strong>in</strong> an adult population: The Pacific Northwest<br />
Bell Telephone Company Health Survey. Atherosclerosis<br />
1981:39:133-146<br />
8. Hoover JJ, Walden CE, Bergelln RO, et al. Cholesterol <strong>and</strong><br />
triglyceride distributions <strong>in</strong> an adult employee population: The<br />
Pacific Northwest Bell Telephone Company Health Survey.<br />
<strong>Lipids</strong> 1980:15:895-903<br />
9. Lipid Research Cl<strong>in</strong>ics Program. Manual of laboratory operations,<br />
Vol 1: Upid <strong>and</strong> lipoprote<strong>in</strong> analysis. (DHEW pub.<br />
no. (NIH) 75-628. Wash<strong>in</strong>gton, DC: U.S. Government Pr<strong>in</strong>t<strong>in</strong>g<br />
Office, 1974<br />
10. Hatch FT, Lees RS. Practical methods for plasma lipoprote<strong>in</strong><br />
analysis. In: Paoletti R, Kritchevsky R, eds. Advanced Upid<br />
Research, vol 6. 1968:1-68<br />
11. Albers JJ, Cabana VG, Hazzard WR. Immunoassay of human<br />
plasma apolipoprote<strong>in</strong> B. Metabolism 1975:24:1339-<br />
1351
PREGNANCY HYPERLIPIDEMIA AND PRELIPEMIA Montes et al. 417<br />
12. Albers JJ, Wahl PW, Cabana VG, Hazzard WR, Hoover JJ.<br />
Quantitation of apolipoprote<strong>in</strong> A-l of human plasma high density<br />
lipoprote<strong>in</strong>. Metabolism 1976;25:633-644<br />
13. Siegel S. Nonparametric statistics for the behavioral sciences.<br />
New York: McGraw-Hill, 1956:520<br />
14. Humphrey JL, Childs MT, Montes A, Knopp RH. Lipid metabolism<br />
<strong>in</strong> pregnancy. VII. K<strong>in</strong>etics of chylomicron triglyceride<br />
removal <strong>in</strong> fed pregnant rat. Am J Physiol 1980;239:E81-<br />
87<br />
15. Childs MT, Tollefson J, Knopp RH, Applebaum-Bowden<br />
D. Lipid metabolism <strong>in</strong> pregnancy. VIII. Effects of dietary fat<br />
vs. carbohydrate on lipoprote<strong>in</strong> <strong>and</strong> hepatic lipids <strong>and</strong> tissue<br />
triglyceride lipases. Metabolism 1981;30:27-35<br />
16. Knopp RH, Montes A, Childs M, Li J. Metabolic adjustments<br />
<strong>in</strong> normal <strong>and</strong> diabetic pregnancy. Cl<strong>in</strong> Obstet Gynecol<br />
17. Childs MT, Knopp RH. Role of diet <strong>in</strong> the hyperiipidemia of<br />
pregnancy, [abstr] Fed Proc 1978;37:348<br />
18. Chan L, Jackson RL, O'Malley B, Means AR. Synthesis of<br />
very low density lipoprote<strong>in</strong>s <strong>in</strong> the cockerel. J Cl<strong>in</strong> Invest<br />
1976;58:368-379<br />
19. Wilson DE, Lees RS. Metabolic relationships among the<br />
plasma lipoprote<strong>in</strong>s: Reciprocal changes <strong>in</strong> the concentrations<br />
of very low, <strong>and</strong> low density lipoprote<strong>in</strong>s <strong>in</strong> man. J Cl<strong>in</strong><br />
Invest 1972;51:1051-1057<br />
20. Chait A, Albers J J, Brunzell JD. Very low density lipoprote<strong>in</strong><br />
over production <strong>in</strong> genetic forms of hypertriglyceridemia. Eur<br />
J Cl<strong>in</strong> Invest 1979;10:17-22<br />
21. Goldste<strong>in</strong> JL, Schrott HG, Hazzard WR, Bierman EL, Motulsky<br />
AG. Hyperiipidemia <strong>in</strong> coronary heart disease. II. Genetic<br />
analysis of lipid levels <strong>in</strong> 176 families <strong>and</strong> del<strong>in</strong>eation of<br />
a new <strong>in</strong>herited disorder, comb<strong>in</strong>ed hyperiipidemia. J Cl<strong>in</strong><br />
Invest 1973:52:1544-1568<br />
22. Walden CE, Wahl PW, Knopp RH, et al. Hyperiipidemia <strong>in</strong><br />
the Pacific Northwest Bell Telephone Company Health Survey:<br />
Part I: Lipoprote<strong>in</strong> cholesterol <strong>and</strong> triglyceride concentrations.<br />
Arteriosclerosis 1983:3:117-124<br />
23. Walden CE, Knopp RH, Wahl PW, et al. Hyperiipidemia <strong>in</strong><br />
the Pacific Northwest Bell Telephone Company Health Survey:<br />
Part II: Lipoprote<strong>in</strong> lipid <strong>in</strong>terrelationships. Arteriosclerosis<br />
1983:3:125-131<br />
24. Hillman L, Schonfeld G, Miller JP, Wolff G. Apoliprote<strong>in</strong>s <strong>in</strong><br />
human pregnancy. Metabolism 1975:24:943-952<br />
25. Warth MR, Arky RA, Knopp RH. Lipid metabolism <strong>in</strong> pregnancy.<br />
III. Altered lipid composition <strong>in</strong> <strong>in</strong>termediate, very low,<br />
low <strong>and</strong> high density lipoprote<strong>in</strong> fractions. J Cl<strong>in</strong> Endocr<strong>in</strong>ol<br />
Metab 1975;41:649-655<br />
26. Schonfeld G, Pf leger B. The structure of human high density<br />
lipoprote<strong>in</strong> <strong>and</strong> the levels of apoprote<strong>in</strong> Al <strong>in</strong> plasma as determ<strong>in</strong>ed<br />
by radioimmunoassay. J Cl<strong>in</strong> Invest 1974;54:236-246<br />
27. Glueck CJ, Christopher C, Tsang RC, Mellies MJ. Cholesterol-free<br />
diet <strong>and</strong> the physiologic hyperiipidemia of pregnancy<br />
<strong>in</strong> familial hypercholesterolemia. Metabolism 1980;<br />
29:949-955<br />
28. McMurry MP, Connor WE, Goplerud CP. The effects of<br />
dietary cholesterol upon the hypercholesterolemia of pregnancy.<br />
Metabolism 1981;30:869-879<br />
29. Sniderman A, Shapiro S, Marpole D, Sk<strong>in</strong>ner B, Teng B,<br />
Kwiterovich P. Association of coronary atherosclerosis with<br />
hyperapobetalipoprote<strong>in</strong>emia. Proc Natl Acad Sci USA 1980;<br />
77:604-608<br />
30. Tall AR, Small DM, Atk<strong>in</strong>son D, Rudel LL. Studies on the<br />
structure of low density lipoprote<strong>in</strong>s from Macaca fascicularis<br />
fed an atherogenic diet. J Cl<strong>in</strong> Invest 1978:62:1354-1363<br />
31. Bengtsson C, Rybo G, Westerberg H. Number of pregnancies,<br />
use of contraceptives, <strong>and</strong> menopausal age <strong>in</strong> women<br />
with ischemic heart disease, compared to a population sample<br />
of women. Acta Med Sc<strong>and</strong> (Suppl) 1973:549:75-81<br />
Index Terms, lipoprote<strong>in</strong>s • apoprote<strong>in</strong>s • pregnancy • hyperiipidemia • prelipemia<br />
Downloaded from<br />
http://atvb.ahajournals.org/ by guest on June 29, 2013