Sacral neuromodulation for the treatment of refractory urinary urge ...
Sacral neuromodulation for the treatment of refractory urinary urge ...
Sacral neuromodulation for the treatment of refractory urinary urge ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
American Journal <strong>of</strong> Obstetrics and Gynecology (2005) 193, 2083–7<br />
<strong>Sacral</strong> <strong>neuromodulation</strong> <strong>for</strong> <strong>the</strong> <strong>treatment</strong> <strong>of</strong><br />
<strong>refractory</strong> <strong>urinary</strong> <strong>urge</strong> incontinence after<br />
stress incontinence s<strong>urge</strong>ry<br />
Neil D. Sherman, MD, a, * Margaret G. Jamison, PhD, b George D. Webster, MB, FRCS, a<br />
Cindy L. Amundsen, MD a,b<br />
Divisions <strong>of</strong> Urology, a Urogynecology, b Duke University Medical Center, Durham, NC<br />
Received <strong>for</strong> publication January 14, 2005; revised June 8, 2005; accepted July 5, 2005<br />
KEY WORDS<br />
<strong>Sacral</strong><br />
<strong>neuromodulation</strong><br />
Interstim <strong>the</strong>rapy<br />
Overactive bladder<br />
symptoms<br />
Stress <strong>urinary</strong><br />
incontinence<br />
Pubovaginal sling<br />
Urinary incontinence<br />
<strong>the</strong>rapy<br />
A variety <strong>of</strong> surgical techniques report a greater than<br />
80% cure rate in treating <strong>urinary</strong> stress incontinence. 1,2 In<br />
addition, surgical intervention <strong>for</strong> stress incontinence<br />
may help <strong>the</strong> symptoms <strong>of</strong> <strong>the</strong> overactive bladder<br />
Presented at <strong>the</strong> 31st Annual Meeting <strong>of</strong> <strong>the</strong> Society <strong>of</strong> Gynecologic<br />
S<strong>urge</strong>ons Annual Scientific Meeting, April 4-6, 2005, Rancho Mirage, CA.<br />
* Reprint requests: Neil D. Sherman, MD, Duke University Medical<br />
Center, Division <strong>of</strong> Urology, DUMC 3146, Durham, NC 27710.<br />
E-mail: neil.sherman@duke.edu<br />
0002-9378/$ - see front matter Ó 2005 Mosby, Inc. All rights reserved.<br />
doi:10.1016/j.ajog.2005.07.038<br />
www.ajog.org<br />
Objective: This study was undertaken to evaluate <strong>the</strong> response to sacral <strong>neuromodulation</strong> in<br />
women with <strong>refractory</strong>, nonobstructive <strong>urinary</strong> <strong>urge</strong> incontinence after stress incontinence s<strong>urge</strong>ry.<br />
Study design: We reviewed <strong>the</strong> medical records <strong>of</strong> women in whom sacral <strong>neuromodulation</strong> was<br />
per<strong>for</strong>med <strong>for</strong> worsening or de novo <strong>urinary</strong> <strong>urge</strong> incontinence after a stress incontinence<br />
procedure. All patients had undergone preliminary test stimulation. Demographics, surgical and<br />
urogynecologic history, including bladder diary and pad weight test, and urodynamic parameters<br />
were evaluated.<br />
Results: Of 34 women, 22 (65%) responded to <strong>the</strong> test stimulation and underwent permanent lead<br />
implant. There was no difference between responders and nonresponders with respect to type <strong>of</strong><br />
stress incontinence s<strong>urge</strong>ry. Incontinence or urodynamic parameters were not different between<br />
responders and nonresponders. Factors that were predictive <strong>of</strong> a positive response were women<br />
aged less than 55 years (P = .01), <strong>the</strong> test stimulation per<strong>for</strong>med within 4 years <strong>of</strong> <strong>the</strong> stress<br />
incontinence procedure (P = .01), and evidence <strong>of</strong> pelvic floor muscle activity (P = .03).<br />
Conclusion: <strong>Sacral</strong> <strong>neuromodulation</strong> is a viable option <strong>for</strong> <strong>the</strong> <strong>treatment</strong> <strong>of</strong> <strong>refractory</strong> <strong>urinary</strong> <strong>urge</strong><br />
incontinence that occurs after stress <strong>urinary</strong> incontinence s<strong>urge</strong>ry. Older women with no pelvic<br />
floor activity who are remote from <strong>the</strong>ir incontinence s<strong>urge</strong>ry may have a suboptimal response.<br />
Ó 2005 Mosby, Inc. All rights reserved.<br />
(OAB) in women with mixed incontinence. 3,4 However,<br />
it is estimated that de novo <strong>urinary</strong> <strong>urge</strong> incontinence<br />
(UUI) occurs in 10% <strong>of</strong> women after stress <strong>urinary</strong><br />
incontinence (SUI) s<strong>urge</strong>ry and up to 40% <strong>of</strong> women<br />
will have persistent UUI. 5,6<br />
The accepted <strong>treatment</strong> algorithm <strong>for</strong> women with<br />
postsurgical <strong>urinary</strong> frequency, <strong>urge</strong>ncy, and <strong>urge</strong> incontinence<br />
is similar to that used in idiopathic OAB<br />
and includes behavioral <strong>the</strong>rapy and pharmaco<strong>the</strong>rapy.<br />
Although anticholinergic medication reduces <strong>urge</strong>
2084 Sherman et al<br />
incontinent episodes and voiding frequency, many are<br />
not improved significantly. 7 In <strong>the</strong> past, those with<br />
<strong>refractory</strong> <strong>urge</strong>ncy, frequency, and <strong>urge</strong> incontinence<br />
ei<strong>the</strong>r accepted <strong>the</strong>ir condition or underwent sling takedown<br />
or revision, augmentation cystoplasty, detrusor<br />
myomectomy, or denervation procedures.<br />
Recently, patients with intractable UUI, <strong>urge</strong>ncyfrequency,<br />
or nonobstructive <strong>urinary</strong> retention have<br />
been reported to show improvement after undergoing<br />
sacral <strong>neuromodulation</strong> (InterStim Continence Control<br />
System, Medtronic, Inc, Minneapolis, MN). 8 To date,<br />
<strong>the</strong> efficacy <strong>of</strong> sacral <strong>neuromodulation</strong> has not been<br />
reported in women who underwent SUI s<strong>urge</strong>ry and<br />
who have de novo or worsening UUI develop.<br />
In this study, we look at <strong>the</strong> use <strong>of</strong> sacral <strong>neuromodulation</strong><br />
<strong>for</strong> <strong>the</strong> <strong>treatment</strong> <strong>of</strong> <strong>refractory</strong> UUI after<br />
stress incontinence s<strong>urge</strong>ry. We also examine whe<strong>the</strong>r<br />
demographic or pretest stimulation variables predict<br />
a positive response to sacral <strong>neuromodulation</strong>.<br />
Material and methods<br />
Institutional review board approval was obtained <strong>for</strong> this<br />
retrospective analysis. The medical records <strong>of</strong> all women<br />
undergoing sacral <strong>neuromodulation</strong> test-stimulation between<br />
October 2000 and September 2004 were reviewed.<br />
Those with severe OAB symptoms, which appeared de<br />
novo or persisted or worsened after <strong>the</strong>ir stress incontinence<br />
s<strong>urge</strong>ry, were eligible <strong>for</strong> this study. All had been<br />
referred to our Female Urology and Urogynecology clinic<br />
because <strong>of</strong> <strong>the</strong> severity <strong>of</strong> <strong>the</strong>ir OAB symptoms and<br />
having failed behavioral <strong>the</strong>rapy, pelvic floor re-education,<br />
and anticholinergic <strong>treatment</strong>. Their evaluation<br />
included completion <strong>of</strong> a urogynecologic questionnaire,<br />
a pelvic examination with assessment <strong>of</strong> pelvic floor<br />
muscle strength based on a modified, validated pelvic<br />
floor muscle grading system, 9 a 3-day bladder diary<br />
recording micturition frequency, voided volumes and<br />
incontinent episodes (IE) per day, a 24-hour pad weight<br />
test, cystoscopy, and a video-urodynamic study. Women<br />
with urethral obstruction, based on evidence <strong>of</strong> a retropexed<br />
urethra on pelvic examination, poor sagital rotation<br />
<strong>of</strong> <strong>the</strong> urethra during cystoscopy, and/or obstruction<br />
on <strong>the</strong> micturition study underwent urethrolysis or incision<br />
and release <strong>of</strong> <strong>the</strong>ir sling. Nonobstructed women<br />
were candidates <strong>for</strong> a test stimulation because <strong>of</strong> <strong>the</strong><br />
severity <strong>of</strong> <strong>the</strong>ir symptoms and unresponsiveness to<br />
medical and behavioral <strong>the</strong>rapy.<br />
Similar criteria were used <strong>for</strong> our study cohort as is<br />
used when <strong>of</strong>fering sacral <strong>neuromodulation</strong> in previously<br />
studied InterStim groups. Be<strong>for</strong>e <strong>of</strong>fering a test<br />
stimulation, all women underwent extensive pelvic floor<br />
re-education and had tried at least 2 anticholinergic<br />
medications to improve <strong>the</strong>ir symptoms. Those women<br />
with less than a 50% improvement in <strong>the</strong>ir symptoms<br />
and still requiring <strong>the</strong> use <strong>of</strong> multiple protective pads per<br />
day because <strong>of</strong> UUI were <strong>of</strong>fered a test stimulation. The<br />
test stimulation period lasted between 5 and 7 days and<br />
was per<strong>for</strong>med ei<strong>the</strong>r as an outpatient procedure via a<br />
percutaneous electrode (PNE) or a 2-stage approach as<br />
previously described. 10,11<br />
During <strong>the</strong> testing period, women completed a bladder<br />
diary recording voiding frequency, voided volumes,<br />
IE per day, severity <strong>of</strong> leakage, and number <strong>of</strong> pads<br />
used. In addition, a 24-hour pad weight test was<br />
collected <strong>the</strong> day be<strong>for</strong>e evaluation. A positive response<br />
was defined as a 50% or more improvement in baseline<br />
<strong>urge</strong> incontinent episodes or a 50% or more reduction in<br />
pad weight during <strong>the</strong> testing period. All positive<br />
responders were <strong>of</strong>fered permanent implantation. Permanent<br />
implantation consisted <strong>of</strong> a tined lead placed in<br />
<strong>the</strong> S3 sacral <strong>for</strong>amen that was connected to a pulse<br />
generator implanted in <strong>the</strong> fatty tissue <strong>of</strong> <strong>the</strong> buttock.<br />
Age, time since incontinence s<strong>urge</strong>ry, and urodynamic<br />
measurements, all continuous variables, were changed to<br />
categorical variables with 2 responses (age older than 55<br />
years and age 55 years or less) that best discriminated<br />
between responders and nonresponders. Two-way c 2<br />
tests were computed between <strong>the</strong>se variables and responders<br />
and nonresponders, young responders and older<br />
responders, and older respondents and older nonresponders.<br />
A logistic regression model was created to<br />
find which independent variable(s) best predicted response<br />
or nonresponse in <strong>the</strong> older age group because<br />
<strong>the</strong>re were no nonresponders in <strong>the</strong> younger age group.<br />
Results<br />
A total <strong>of</strong> 107 women underwent sacral <strong>neuromodulation</strong><br />
test stimulation between October 2000 and September<br />
2004. Of <strong>the</strong> 107 women tested whose OAB<br />
symptoms appeared de novo or persisted or worsened<br />
after <strong>the</strong>ir stress incontinence s<strong>urge</strong>ry, 34 (32%) were<br />
included in <strong>the</strong> study.<br />
Of <strong>the</strong> 34 women in this study cohort, 22 (65%)<br />
responded to <strong>the</strong> sacral <strong>neuromodulation</strong> test stimulation<br />
and all had a permanent lead and pulse generator implanted.<br />
Twelve patients (35%) did not have greater than<br />
a 50% improvement in incontinent episodes or greater<br />
than 50% reduction in pad weights during <strong>the</strong> testing<br />
period and were classified as nonresponders, and <strong>the</strong>re<strong>for</strong>e<br />
were not implanted. There were no o<strong>the</strong>r alternative<br />
<strong>the</strong>rapies or surgical <strong>treatment</strong>s <strong>of</strong>fered to <strong>the</strong>se 12 nonresponders.<br />
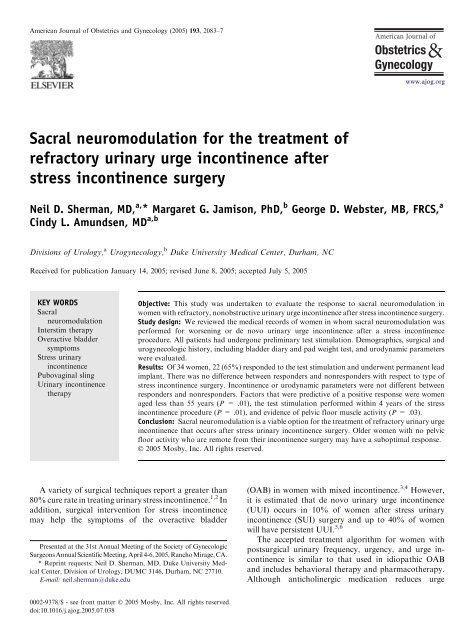
The average age <strong>of</strong> <strong>the</strong> responders was 58 (range 35-82<br />
years) and 66 (range 56-80 years) <strong>for</strong> <strong>the</strong> nonresponders<br />
(Figure). There was a difference between <strong>the</strong> responders<br />
and nonresponders with respect to age and length <strong>of</strong> time<br />
from incontinence s<strong>urge</strong>ry to <strong>the</strong> test stimulation. All <strong>the</strong><br />
nonresponders were older than 55 years and 62% were<br />
4 or more years from <strong>the</strong>ir incontinence s<strong>urge</strong>ry. Type<br />
<strong>of</strong> stress incontinence s<strong>urge</strong>ry and whe<strong>the</strong>r a sling incision
Sherman et al 2085<br />
Table I Surgical history <strong>of</strong> responders versus nonresponders<br />
Characteristics N Responders (%) Nonresponders (%) P-value<br />
Age O55 y 34 59.1 100.0 .01<br />
Time since incontinence s<strong>urge</strong>ry (O4 y) 30 13.6 62.5 .01<br />
Incontinence s<strong>urge</strong>ries 34<br />
PVS 8 22.7 25.0<br />
PVS and prolapse repair 10 31.8 25.0 .95<br />
PVS and sling incision 9 27.3 25.0<br />
O<strong>the</strong>r: 7 18.2 25.0<br />
Burch (with repair) 3<br />
Collagen 3<br />
Needle suspension<br />
PVS, Pubovaginal sling.<br />
1<br />
and release was per<strong>for</strong>med were not statistically significant<br />
factors between responders and nonresponders<br />
(Table I).<br />
Because a younger age has been previously shown to<br />
be an independent variable <strong>for</strong> success with sacral<br />
<strong>neuromodulation</strong> 7 and this was reproduced in our study,<br />
we re-evaluated previously determined variables using<br />
<strong>the</strong> age <strong>of</strong> 55 as a cut<strong>of</strong>f between <strong>the</strong> 2 groups. The only<br />
parameter that was statistically significant between <strong>the</strong><br />
2 groups was that women older than 55, who responded<br />
to sacral <strong>neuromodulation</strong>, had more IE per day than<br />
<strong>the</strong> younger responders. All urodynamic and incontinence<br />
symptom parameters were similar. Interestingly,<br />
whe<strong>the</strong>r <strong>the</strong> woman was young or old, few responded to<br />
sacral <strong>neuromodulation</strong> if <strong>the</strong>ir s<strong>urge</strong>ry had been<br />
per<strong>for</strong>med more than 4 years be<strong>for</strong>e <strong>the</strong> test stimulation<br />
procedure (Table II).<br />
All <strong>the</strong> nonresponders were in <strong>the</strong> group <strong>of</strong> women<br />
older than 55 years. When one compared this older<br />
group <strong>of</strong> responders and nonresponders, lack <strong>of</strong> pelvic<br />
floor muscular activity best correlated with nonresponding<br />
to sacral <strong>neuromodulation</strong> (Table III). After logistic<br />
regression, if <strong>the</strong> woman is older than 55 years with no<br />
pelvic floor activity, she has a 100% chance <strong>of</strong> not<br />
responding to sacral <strong>neuromodulation</strong> in this cohort <strong>of</strong><br />
women (Table IV).<br />
Comment<br />
The incidence <strong>of</strong> OAB symptoms after SUI s<strong>urge</strong>ry<br />
depends on <strong>the</strong> surgical technique used, and can be as<br />
high as 31%, although usually less than 10%. 12-15 Even<br />
with <strong>the</strong> newer minimally invasive approaches <strong>for</strong> stress<br />
incontinence, <strong>the</strong> risk <strong>of</strong> OAB symptoms postoperatively<br />
persists. In this study, 7 <strong>of</strong> <strong>the</strong> 28 slings were<br />
placed by using a minimally invasive technique. Although<br />
SUI may be resolved, <strong>the</strong> presence <strong>of</strong> OAB<br />
symptoms proves to be a source <strong>of</strong> continued patient<br />
dissatisfaction after incontinence procedures. 13,16<br />
It is not clear why OAB symptoms sometimes occur<br />
after stress incontinence procedures. Possible causes<br />
Figure Age distribution <strong>of</strong> responders and non-responders.<br />
include undiscovered preexisting detrusor overactivity,<br />
a neurogenic dysfunction resulting from surgical interference<br />
with autonomic bladder innervation, increased<br />
striated urethral sphincter activity, or structural urethral<br />
obstruction. 17-20 In <strong>the</strong> latter, sling incision and revision<br />
or o<strong>the</strong>r urethrolysis procedures are considered. In <strong>the</strong>se<br />
cases, postoperative voiding symptoms (frequency, <strong>urge</strong>ncy,<br />
and <strong>urge</strong> incontinence) occur in conjunction with<br />
<strong>the</strong> finding <strong>of</strong> a retropexed urethra and/or an obstructive<br />
voiding pattern on urodynamics. One third <strong>of</strong> <strong>the</strong><br />
women in our study group had undergone sling release<br />
that had relieved obstructive voiding symptoms but<br />
OAB symptoms had persisted. Interestingly, having had<br />
a sling incision and release did not affect response to<br />
<strong>neuromodulation</strong>.<br />
The mechanism by which <strong>neuromodulation</strong> works<br />
is not completely understood, it has been shown to be<br />
efficacious in idiopathic <strong>refractory</strong> <strong>urge</strong> incontinence<br />
and nonobstructive <strong>urinary</strong> retention. 6,21 It is believed<br />
that <strong>neuromodulation</strong> treats bladder overactivity by<br />
altering <strong>the</strong> activity and basal tone <strong>of</strong> <strong>the</strong> pelvic floor<br />
as well as modulating <strong>the</strong> afferent signals delivered to<br />
<strong>the</strong> spinal cord. 22 The cause <strong>of</strong> nonobstructive <strong>urinary</strong>
2086 Sherman et al<br />
Table II Comparison <strong>of</strong> surgical, incontinence, and urodynamic<br />
parameters between younger and older respondents<br />
Young Older<br />
responders responders P-<br />
Measurements N (%) (%) value<br />
Time since incontinence<br />
s<strong>urge</strong>ry (O4 y)<br />
20 25.0 33.3 .69<br />
Pelvic floor muscle %2 20 37.5 41.6 .85<br />
Prepad weight (g) O400 20 50.0 50.0 .99<br />
Incontinence episodes<br />
(no.) O5<br />
20 12.5 66.7 .02<br />
Pads/day (no.) R5 20 62.5 50.0 .58<br />
Void volume (mL) R150 20 75.0 75.0 .99<br />
Frequency (no. voids/<br />
day) O10<br />
20 50.0 50.0 .99<br />
Pdet@Qmax<br />
(cm H2O) O20<br />
9 60.0 50.0 .76<br />
Flow rate (mL/s) !12 11 57.1 50.0 .99<br />
Presence <strong>of</strong> detrusor<br />
overactivity<br />
19 71.4 50.0 .36<br />
Pdet@Qmax, Detrusor pressure (cm H2O) at maximum flow (mL/<br />
second).<br />
Table III Comparison <strong>of</strong> surgical, incontinence, and urodynamic<br />
measurements <strong>for</strong> older respondents and nonrespondents<br />
Older Older non<br />
responders responders P-<br />
Measurements N (%) (%) value<br />
Time since incontinence<br />
s<strong>urge</strong>ry (O4 y)<br />
21 15.4 62.5 .03<br />
Pelvic floor muscle %2 21 15.4 62.4 .03<br />
Prepad weight (g) O400 21 38.5 75.0 .10<br />
IE/day (no.) O5 21 61.5 50.0 .60<br />
Pads/day (no.) R5 21 69.2 25.0 .05<br />
Void volume (mL) R150 20 50.0 87.5 .09<br />
Frequency (no.<br />
voids/day) O10<br />
20 50.0 37.5 .58<br />
Pdet@Qmax<br />
(cm H2O) O20<br />
11 50.0 80.0 .30<br />
Flow rate (mL/s) !12 11 60.0 33.3 .38<br />
Presence <strong>of</strong> detrusor<br />
overactivity<br />
21 69.2 62.5 .75<br />
retention is believed to be due to a primary failure <strong>of</strong><br />
relaxation <strong>of</strong> <strong>the</strong> striated urethral sphincter. 19,23 The<br />
mechanism <strong>of</strong> action <strong>for</strong> <strong>neuromodulation</strong> in retention<br />
patients is believed to be an activation <strong>of</strong> somatic<br />
afferent axons in <strong>the</strong> sacral spinal roots causing an<br />
inhibition <strong>of</strong> reflex pathways to <strong>the</strong> urethral outlet. This<br />
ultimately relieves pelvic floor spasticity, releasing <strong>the</strong><br />
detrusor from inhibition to allow <strong>for</strong> spontaneous<br />
voiding. 24<br />
Table IV Nonrespondent rates <strong>for</strong> age and pelvic muscle<br />
floor measurements<br />
Percentage<br />
Factor<br />
nonresponse<br />
Age alone<br />
O55 y 48% nonresponse<br />
PFM alone<br />
PFM = 0 or 1 80% nonresponse<br />
PFM %2 50% nonresponse<br />
Age and PFM in combination<br />
PFM = 0 or 1 and Age O55 y 100% nonresponse<br />
PFM %2 and Age O55 y 71% nonresponse<br />
PFM, Pelvic floor measurement.<br />
In this study, <strong>the</strong> overall response to sacral <strong>neuromodulation</strong><br />
is similar to that which is reported by o<strong>the</strong>r<br />
groups treating <strong>refractory</strong> idiopathic <strong>urge</strong> incontinence<br />
with <strong>neuromodulation</strong>. 22 There are no pretest stimulation<br />
urodynamic variables to predict success <strong>of</strong> sacral<br />
<strong>neuromodulation</strong> and similarly in this cohort no urodynamic<br />
variables seemed predictative <strong>of</strong> success. This<br />
study duplicates our earlier results, specifically, that<br />
younger women responded better to sacral <strong>neuromodulation</strong>.<br />
7 In addition, <strong>the</strong> presence <strong>of</strong> pelvic floor neuromuscular<br />
activity, evaluated by voluntarily contracting<br />
<strong>the</strong> pelvic floor, was also found to predict a positive<br />
response to <strong>neuromodulation</strong> in our cohort. Because <strong>the</strong><br />
believed mechanism <strong>of</strong> action <strong>of</strong> sacral <strong>neuromodulation</strong><br />
relies on afferent input from <strong>the</strong> pelvic floor, this<br />
might explain <strong>the</strong> better response in <strong>the</strong>se women<br />
compared with those who demonstrated no voluntary<br />
pelvic floor muscle contractile ability.<br />
Our data show that a short duration between stress<br />
incontinence s<strong>urge</strong>ry and sacral <strong>neuromodulation</strong> was<br />
predictive <strong>of</strong> a positive response to <strong>neuromodulation</strong> in<br />
both <strong>the</strong> younger and older groups. There may be<br />
unidentified pathologic or neurologic bladder changes<br />
that occur and limit success when time to intervention is<br />
prolonged.<br />
This is a small cohort study and findings regarding<br />
correlation with time from s<strong>urge</strong>ry, pelvic floor muscle<br />
denervation, and age need to be confirmed with a larger<br />
cohort. Our results have led us to <strong>of</strong>fer test stimulation <strong>for</strong><br />
sacral <strong>neuromodulation</strong> to women who have <strong>refractory</strong><br />
OAB symptoms after a SUI procedure. Never<strong>the</strong>less,<br />
older women with no pelvic floor activity who are remote<br />
from <strong>the</strong>ir incontinence s<strong>urge</strong>ry may be counseled to a<br />
probable suboptimal response.<br />
Conclusion<br />
Response to sacral <strong>neuromodulation</strong> <strong>for</strong> <strong>the</strong> <strong>treatment</strong><br />
<strong>of</strong> <strong>refractory</strong> <strong>urge</strong> incontinence after SUI s<strong>urge</strong>ry is<br />
comparable to its use in idiopathic <strong>urge</strong> incontinence.
Sherman et al 2087<br />
The type <strong>of</strong> stress incontinence s<strong>urge</strong>ry, incontinence<br />
parameters, and preimplantation urodynamics do not<br />
help predict response to <strong>neuromodulation</strong>. Our study<br />
suggests that a younger age, a shorter time from <strong>the</strong><br />
incontinence s<strong>urge</strong>ry and evidence <strong>of</strong> pelvic floor muscular<br />
activity appear to predict a better response. <strong>Sacral</strong><br />
<strong>neuromodulation</strong> should be considered in women with<br />
severe OAB symptoms after SUI s<strong>urge</strong>ry having failed<br />
medical and behavioral <strong>the</strong>rapy and after urethral<br />
obstruction has been ruled out.<br />
References<br />
1. Leach GE, Dmochowski RR, Appell RA, Blaivas JG, Hadley HR,<br />
Luber KM. Female stress <strong>urinary</strong> incontinence clinical guidelines<br />
panel summary report on surgical management <strong>of</strong> female stress<br />
<strong>urinary</strong> incontinence. J Urol 1997;158:875-80.<br />
2. Jarvis GJ. Stress incontinence. In: Mundy AR, Stephenson TP,<br />
Wein AJ, editors. Urodynamics: principles, practice and<br />
application. 2nd ed. New York: Churchhill Livingston; 1994. p.<br />
299-326.<br />
3. Amundsen CL, Visco AG, Ruiz H, Webster GD. Outcome in 104<br />
pubovaginal slings using freeze-dried allograft fascia lata from a<br />
single tissue bank. Urology 2000;56:2-8.<br />
4. Chou EC, Flisser AJ, Panagopoulos G, Blaivas J. Effective<br />
<strong>treatment</strong> <strong>for</strong> mixed <strong>urinary</strong> incontinence with a pubovaginal<br />
sling. J Urol Aug 2003;170:494-7.<br />
5. Kobashi KC, Leach GE, Chon J, Govier FE. Continued multicenter<br />
followup <strong>of</strong> cadaveric prolapse repair with sling. J Urol<br />
2002;168:2063-8.<br />
6. Frederick RW, Carey JM, Leach GE. Transvaginal s<strong>urge</strong>ry <strong>for</strong> <strong>the</strong><br />
<strong>treatment</strong> <strong>of</strong> pelvic prolapse and stress incontinence in <strong>the</strong> octogenarian<br />
patient. Issues Incontinence 2004;S/S:3-9.<br />
7. Diokno AC, Appell RA, Sand PK, Dmochowski RR, Gburek BM,<br />
Klimberg IW, et al. Prospective, randomized, double-blind study<br />
<strong>of</strong> <strong>the</strong> efficacy and tolerability <strong>of</strong> <strong>the</strong> extended-release <strong>for</strong>mulations<br />
<strong>of</strong> oxybutynin and tolterodine <strong>for</strong> overactive bladder: results <strong>of</strong> <strong>the</strong><br />
OPERA trial. The OPERA Study Group. Mayo Clin Proc<br />
2003;78:687-95.<br />
8. Siegel SW, Catanzaro F, Dijkema HE, Elhilali MM, Fowler CJ,<br />
Gajewski JB, et al. Long-term results <strong>of</strong> a multicenter study on<br />
sacral nerve stimulation <strong>for</strong> <strong>treatment</strong> <strong>of</strong> <strong>urinary</strong> <strong>urge</strong> incontinence,<br />
<strong>urge</strong>ncy-frequency, and retention. Urology 2000;56(supp<br />
6A):87-91.<br />
9. Brink CA, Wells TJ, Sampselle CM, Taillie ER, Mayer R. A<br />
digital test <strong>for</strong> pelvic muscle strength in women with <strong>urinary</strong><br />
incontinence. Nurs Res 1994;43:352-6.<br />
10. Amundsen CL, Webster GD. <strong>Sacral</strong> <strong>neuromodulation</strong> in an older,<br />
<strong>urge</strong>-incontinent population. Am J Obstet Gynecol 2002;187:<br />
1462-5.<br />
11. Janknegt RA, Weil EHJ, Eerdmans PHA. Improving <strong>neuromodulation</strong><br />
technique <strong>for</strong> <strong>refractory</strong> voiding dysfunctions: twostage<br />
implant. Urology 1997;49:358-62.<br />
12. Wang AC. Burch colposuspension vs. Stamey bladder neck<br />
suspension: a comparison <strong>of</strong> complications with special emphasis<br />
on detrusor instability and voiding dysfunction. J Reprod Med<br />
1996;41:529-33.<br />
13. Deval B, Jeffry L, Al Najjar F, Soriano D, Darai E. Determinants<br />
<strong>of</strong> patient dissatisfaction after a tension-free vaginal tape procedure<br />
<strong>for</strong> <strong>urinary</strong> incontinence. J Urol May 2002;167:2093-7.<br />
14. Arunkalaivanan AS, Barrington JW. Randomized trial <strong>of</strong> porcine<br />
dermal sling (Pelvicol implant) vs. tension-free vaginal tape (TVT)<br />
in <strong>the</strong> surgical <strong>treatment</strong> <strong>of</strong> stress incontinence: a questionnairebased<br />
study. Int Urogynecol J 2003;14:17-23.<br />
15. Chaikin DC, Rosenthal J, Blaivas JG. Pubovaginal fascial sling <strong>for</strong><br />
all types <strong>of</strong> stress <strong>urinary</strong> incontinence: long-term analysis. J Urol<br />
1998;160:1312-6.<br />
16. Ful<strong>for</strong>d SCV, Flynn R, Barrington J, Appanna T, Stephenson TP.<br />
An assessment <strong>of</strong> <strong>the</strong> surgical outcome and urodynamic effects <strong>of</strong><br />
<strong>the</strong> pubovaginal sling <strong>for</strong> stress incontinence and <strong>the</strong> associated<br />
<strong>urge</strong> syndrome. J Urol 1999;162:135-7.<br />
17. Sand PK, Bowen LW, Osyergard DR, Brubaker L, Panganiban R.<br />
The effects <strong>of</strong> retropubic urethropexy on detrusor instability.<br />
Obstet Gynecol 1988;71:818-22.<br />
18. Cardozo LD, Stanton SL, Williams JE. Detrusor instability<br />
following s<strong>urge</strong>ry <strong>for</strong> genuine stress <strong>urinary</strong> incontinence. Br J<br />
Urol 1979;51:204-7.<br />
19. FitzGerald MP, Brubaker L. The etiology <strong>of</strong> <strong>urinary</strong> retention<br />
after s<strong>urge</strong>ry <strong>for</strong> genuine stress incontinence. Neurourol Urodyn<br />
2001;20:13-21.<br />
20. Leng WW, Davies BJ, Tarin T, Sweeney DD, Chancellor MB.<br />
Delayed <strong>treatment</strong> <strong>of</strong> bladder outlet obstruction after sling s<strong>urge</strong>ry:<br />
association with irreversible bladder dysfunction. J Urol<br />
2004;172:1379-81.<br />
21. Jonas U, Fowler J, Chancellor MB, Elhilali MM, Fall M,<br />
Gajewski JB, et al. Efficacy <strong>of</strong> sacral nerve stimulation <strong>for</strong> <strong>urinary</strong><br />
retention: results 18 months after implantation. J Urol 2001;<br />
165:15-9.<br />
22. Schmidt RA, Jonas U, Oleson KA, Janknegt RA, Hassouna MM,<br />
Siegel SW, et al. <strong>Sacral</strong> nerve stimulation <strong>for</strong> <strong>treatment</strong> <strong>of</strong><br />
<strong>refractory</strong> <strong>urinary</strong> <strong>urge</strong> incontinence. J Urol 1999;62:352-7.<br />
23. Swinn MJ, Oliver J, Wiseman EL, Fowler CJ. The cause and<br />
natural history <strong>of</strong> isolated <strong>urinary</strong> retention in young women.<br />
J Urol 2002;167:151-6.<br />
24. Goodwin RJ, Swinn MJ, Fowler CJ. The neurophysiology <strong>of</strong><br />
<strong>urinary</strong> retention in young women and its <strong>treatment</strong> by <strong>neuromodulation</strong>.<br />
World J Urol 1998;16:305-7.