Keynote Lecture: Fecal Incontinence
Keynote Lecture: Fecal Incontinence
Keynote Lecture: Fecal Incontinence

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Fecal</strong> <strong>Incontinence</strong><br />
The Cleveland Clinic Foundation<br />
Cleveland, Ohio<br />
Tracy L. Hull, M.D.<br />
Professor of Surgery<br />
Digestive Disease Institute<br />
Department of Colorectal Surgery
Several organs in the body were arguing about who was<br />
the most important<br />
• The HEART said it was the most important because it<br />
pumped the blood.<br />
• The BRAIN ‘thought’ it was the most important<br />
because it integrated all information and made<br />
decisions.<br />
• The EYES ‘viewed’ themselves as the most important<br />
because they could tell the body where it was going.<br />
• The KNEES thought they were the most important<br />
because they carried the body where it wanted to go
• Nobody would listen to the ANAL SPHINCTERS<br />
• Therefore they shut down<br />
• After a couple of days of the anus and bowel not<br />
working properly, the eyes went glassy, the<br />
knees buckled, the brain turned to jelly, and the<br />
heart skipped a beat<br />
• Finally they all said “All right ANAL<br />
SPHINCTER, you are the BEST.”
• A normally<br />
functioning anal<br />
sphincter is a gift<br />
from GOD<br />
--anonymous
• Life miserating<br />
• Evaluating<br />
improvement after<br />
treatment is difficult<br />
as no standard<br />
definition for severity<br />
and frequency exists<br />
• Successful outcome is<br />
impossible to define<br />
<strong>Fecal</strong> <strong>Incontinence</strong>
Prevalence based on 16<br />
studies of community<br />
dwelling adults<br />
• Anal incontinence<br />
including flatus 2-24%<br />
• Anal incontinence<br />
(excluding flatal)<br />
0.4-18%<br />
Macmillan et al DCR 2004<br />
<strong>Fecal</strong> <strong>Incontinence</strong>
• Obstetrical injury is<br />
the most common<br />
cause of fecal<br />
incontinence<br />
<strong>Fecal</strong> <strong>Incontinence</strong>
Other Causes<br />
• Surgical trauma (fistulotomy,<br />
hemorrhoidectomy, sphincterotomy)<br />
• Irradiation<br />
• Colitis<br />
• Rectal prolapse<br />
• Central nervous system problems<br />
• Diabetes<br />
• Scleroderma<br />
• Medications<br />
• Others<br />
<strong>Fecal</strong> <strong>Incontinence</strong>
Comprehensive History<br />
• Duration, frequency<br />
• Quality of stool lost<br />
• Flatus control<br />
• Pad use<br />
• Urgency<br />
• Affect on daily life<br />
• Urinary incontinence<br />
<strong>Fecal</strong> <strong>Incontinence</strong><br />
• Obstetric history<br />
• Surgical history<br />
• Other medical problems<br />
• Medications<br />
• Psychosocial<br />
ramifications of<br />
incontinence
Physical exam<br />
• Careful exam of<br />
perineum, anus, and<br />
rectum<br />
Anal ultrasound<br />
• Preferred tool to map<br />
sphincters<br />
• Not always needed but<br />
may be helpful<br />
<strong>Fecal</strong> <strong>Incontinence</strong>
Treatment of <strong>Fecal</strong> <strong>Incontinence</strong><br />
• Treatment options<br />
depend on clear<br />
understanding of<br />
pathophysiology<br />
• Standard treatment starts<br />
with addressing<br />
underlying conditions
Non-Surgical Treatment:<br />
forgotten aspects<br />
• Skin care<br />
• Barrier creams for<br />
protection<br />
• Cotton ball by anus<br />
• Use of baby wipes<br />
<strong>Fecal</strong> <strong>Incontinence</strong>
<strong>Fecal</strong> <strong>Incontinence</strong>: Medical Treatment<br />
• Evaluate and treat diarrhea<br />
• Biofeedback<br />
• Anal plug<br />
• SECCA
<strong>Fecal</strong> <strong>Incontinence</strong>: Medical Treatment<br />
• Evaluate and treat diarrhea<br />
• Biofeedback (pelvic floor<br />
retraining)<br />
• Anal plug<br />
• SECCA
Pelvic Floor Retraining: Biofeedback<br />
• Uses EMG or manometry for visual input<br />
(auditory or visual cue)<br />
• Inexpensive (although many insurance<br />
companies view it as experimental)<br />
• Painless, easy to perform, does not exclude<br />
other tx<br />
• Requires a motivated patient capable of<br />
understanding the treatment AND<br />
MOTIVATED THERAPIST
Biofeedback: Protocols<br />
1. Coordination training—<br />
contract muscle in response to<br />
rectal distension<br />
2. Sensory training—recognize<br />
smaller volumes of rectal<br />
contents<br />
3. Strength training—isolate and<br />
exercise anal muscle (without<br />
rectal distention)
Biofeedback: Outcomes<br />
• N=171 randomized four groups: I) teaching, advice<br />
and support (a), II) + addition of sphincter exercises<br />
(a+b), III) +addition of manometric feedback<br />
(a+b+c), IV) + addition of home training device<br />
(a+b+c+d)<br />
• Continence scores, disease-specific and generic QOL<br />
scores, resting, squeeze, and sustained squeeze<br />
pressures improved in all groups and improvement<br />
was maintained at one year<br />
• Presence and degree of sphincter defect did not<br />
correlate with outcome<br />
Norton Gastroenterology 2003
Biofeedback: Outcomes<br />
• Results vary considerably with reported<br />
success 38-92%<br />
• Success does not diminish in most over time<br />
in few small long term studies (Ryn, Morren 2000)<br />
• May improve function if symptoms persist<br />
w/ successful sphincter repair (Jensen, Lowery 1997)<br />
• No clear patient selection criteria or optimal<br />
protocol
<strong>Fecal</strong> <strong>Incontinence</strong>: Medical Treatment<br />
• Evaluate and treat diarrhea<br />
• Biofeedback<br />
• Anal plug<br />
• SECCA
<strong>Fecal</strong> <strong>Incontinence</strong>: Medical Treatment<br />
• Evaluate and treat diarrhea<br />
• Biofeedback<br />
• Anal plug<br />
• SECCA<br />
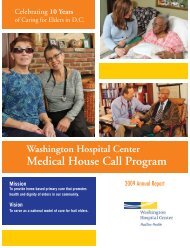
Radio-frequency delivered<br />
to target temperature of 85<br />
C for 1 min 23-32 times in<br />
anal canal
SECCA hand piece<br />
• Anoscopic barrel<br />
SECCA: Equipment<br />
• Light pipe for visualization
SECCA: Procedure<br />
• Goal is four rows 5 mm<br />
apart beginning at the<br />
dentate and moving<br />
proximal (may opt to<br />
treat 5 th row)<br />
• 4 needle treatment per<br />
quadrant<br />
• 85 C for 1 min<br />
• Total 64 lesions
SECCA: How Does it Work?<br />
• Mechanism of action is unknown<br />
• “Radiofrequency anal sphincter remodeling”<br />
(fibroblasts to myoblasts)<br />
• No consistent changes in anal physiology or<br />
anal endosonography
SECCA: First Studies<br />
• Feasibility, safety,<br />
efficacy<br />
• N=10 F/U 12 mos<br />
• Wexner 13.5 to 5<br />
(p
First<br />
author<br />
n F/U<br />
mos<br />
SECCA: Results<br />
Preop<br />
Wexner<br />
Efron<br />
2003 50 6 14<br />
Lefebure<br />
2008<br />
15 12 14<br />
Ruiz<br />
2010 24 12 15<br />
Postop<br />
Wexner<br />
11 Multicenter (5)<br />
prospective all FIQOL sig<br />
improved<br />
12 FIQOL only improved<br />
for depression<br />
12 FIQOL improved in all<br />
subsets except depression
SECCA: not all showed improvement<br />
• N=8 F/U 6 mos<br />
• FISI and FIQOL showed no improvement<br />
(except embarrassment scale)<br />
• 7/8 had anal bleeding, mucous discharge, or<br />
anal pain<br />
Kim Am J Surg 2009
SECCA: Complications<br />
• Bleeding and/or anal pain 10-45%<br />
• Ulceration in 2/50 after Efron study (2003)<br />
led to modification of device<br />
• Potential for rectovaginal fistula<br />
• Local hematoma<br />
• The device inserted is large (?? Sphincter<br />
injury)<br />
• Don’t use SECCA after injectables<br />
• No long term complications reported
SECCA: Final Thoughts<br />
• Consider for Wexner score<br />
9-17 and
Injectables: Types<br />
11 injectable bulking agents in the literature<br />
--- Carbon beads (Durasphere)<br />
--- Teflon<br />
--- Silicone (PTQ R )<br />
--- Collagen<br />
--- Calcium hydroxylapatite (Coaptite R )<br />
--- Fat<br />
---Permacol TM<br />
--- Non-animal Hyaluronic<br />
Acid with Dextranomer (NASHA TM DX<br />
[Solesta R ]))
Injectable Agents<br />
• Injectable stabilized<br />
hyaluronic acid<br />
– n=206 randomized double<br />
blinded sham controlled trial<br />
– 52% >50 % reduction in FI<br />
vs 31% control (p=0.0089)<br />
– One rectal abscess and one<br />
prostatic abscess<br />
Graf et al Lancet 2011
Injectables: Results NASH<br />
• N=34 1 cc x 4 submucosal<br />
• F/U 12 mos for all patients<br />
• FI episodes via 4 wk diary<br />
• Median 10 (r 0-70)<br />
versus pre 22 (r 2-77) (p=0.004)<br />
Danielson Dis Colon Rectum 2009
Injectables: Where and How Much<br />
• 7 different techniques in literature<br />
– Submucosal or intersphincteric space<br />
– Route of needle insertion<br />
• Is ultrasound guidance required<br />
• One cc in four quadrants<br />
• Size of needle to implant (21 gauge)
Injectables: Final Thoughts<br />
• We have minimal evidence-based information<br />
to guide us regarding injectables<br />
• Where to inject; what route; how much???<br />
• Are laxatives important?<br />
• Would we improve results if done in OR?<br />
• RCT with sufficient number of patients<br />
and longer F/U needed
<strong>Fecal</strong> <strong>Incontinence</strong>: Surgical Treatment<br />
• Overlapping sphincter repair<br />
• Sacral Nerve Stimulation<br />
• Artificial bowel sphincter<br />
• ACE<br />
• Stoma<br />
• Not used<br />
Park’s post anal repair<br />
Dynamic graciloplasty
Overlapping Sphincter Repair<br />
• Most common procedure<br />
for repair of anterior defect<br />
ADVANTAGES<br />
• Relatively easy<br />
• Low cost<br />
• No fancy equipment needed<br />
• Can be done globally in any<br />
OR
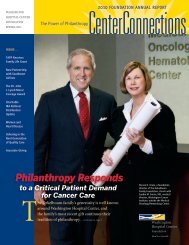
Long-term Results of Overlapping Sphincter Repair<br />
100%<br />
90%<br />
80%<br />
70%<br />
60%<br />
50%<br />
40%<br />
30%<br />
20%<br />
10%<br />
0%<br />
St Marks<br />
2000 n=38<br />
F/U 77 m<br />
France 2000<br />
n=74<br />
F/U 40 m<br />
continent<br />
gas incon<br />
total incon<br />
CCF 2002<br />
n=49<br />
F/U 69 m<br />
U of Minn<br />
2004 n=104<br />
F/U 120 m<br />
CCF 2007<br />
n=41<br />
F/U 126 m
Long Term Outcome Following<br />
Overlapping Sphincter Repair<br />
Why poor long term results?<br />
• ELUS not done to assess<br />
adequate initial repair<br />
• Normal aging of these women’s<br />
muscles?<br />
• Some think fibrosis is more<br />
pronounced in these women and<br />
affects the results<br />
• Unrecognized problem in pelvic<br />
floor
Overlapping Repair: FINAL THOUGHTS<br />
• Long term results of overlapping sphincter<br />
repair may not be as good as previously<br />
assumed<br />
• Overlapping repair of anterior defect is<br />
STILL reasonable treatment
Sacral Nerve Modulation<br />
• 1994 first used for FI<br />
• FDA approved in US<br />
• Adapted from use in<br />
urological disorders<br />
• Unclear mechanism of<br />
action
• 9 Fe 1 M<br />
• PET scan (cerebral blood flow)<br />
– 30 min after continuous stim<br />
started<br />
Sacral Nerve Stimulation<br />
– repeated 2 weeks after<br />
continuous stim<br />
• Initial stim activated contralateral<br />
frontal cortex normally active in<br />
focused attention<br />
Lundby et al Dis Colon Rect 2011
Sacral Nerve Stimulation<br />
• After 2 wks, activation<br />
changed to activity in parts of<br />
ipsilateral caudate nucleus<br />
(thought to be involved in<br />
learning and reward)<br />
• SNS induces changes in<br />
cerebral activity consistent<br />
with effect on afferent<br />
projections of vagus<br />
Lundby et al Dis Colon Rect 2011
Sacral Nerve Stimulation<br />
Indications: FI due to<br />
• Obstetric injury<br />
• Sphincter defect<br />
• Anal trauma<br />
• Cauda equina syndrome<br />
• Rectal resection<br />
• Crohn’s disease with sphincter disruption
Phase 1: Test Stimulation
Phase 2: Implantation of<br />
permanent stimulating device<br />
to the implanted lead
Sacral Nerve Stimulation<br />
Meta-analysis of 34 studies:<br />
• 944 pts with PNE and 665 permanent SNS<br />
• Weekly episodes FI and incontinence scores<br />
significantly reduced<br />
• Ability to defer defecation increased<br />
•
Sacral Nerve Stimulation<br />
Meta-analysis of 34 studies:<br />
• Results similar +/- sphincter defect<br />
• PNE only predictive test for SNS outcome<br />
• Complication rate was 15% for permanent SNS w/<br />
3% having permanent explantation<br />
• Most common complications (n=665): Pain (6%),<br />
lead problem (4%), infection (3%), seroma (3%)<br />
Tan et al Int J Colorectal Dis 2011
Sacral Nerve Stimulation<br />
14 studies + 9 with sphincter lesions all pos<br />
PNE and had permanent implant:<br />
• 77% improvement idiopathic FI<br />
• 76% improvement in sphincter defect (17-180 0 )<br />
• 78% improvement after OSR<br />
• 73% improvement w/ neurologic injury<br />
Matzel Colorectal Dis 2011
Sacral Nerve Stimulation<br />
14 studies + 9 with sphincter lesions all pos<br />
PNE and had permanent implant:<br />
• Sustained benefit at 14 yrs (longest FU)<br />
• Reduction in clinical efficacy with longterm<br />
FU in 26%<br />
Matzel Colorectal Dis 2011
Sacral Nerve Stimulation<br />
Results EAS defect:<br />
• EAS defect (21); intact (32)<br />
• Both had sig improvement QOL<br />
• Weekly FI 13 to 5 (EAS defect<br />
p
Sacral Nerve Stimulation Results<br />
• Pooling data of 8 studies for 238<br />
• Mean F/U16 mos<br />
• 88% of these patients reported >50% improvement<br />
• Complications 5-26% &
Sacral Nerve Modulation Advantages<br />
Advantages of SNS<br />
• Done under local +<br />
sedation<br />
• Not dependant on<br />
sphincter morphology<br />
• Works for SUI ,<br />
? Constipation, ? IBS<br />
• Good results<br />
Disadvantages of SNS<br />
• 30% will not benefit<br />
• % will not be eligible<br />
• 5-26% device related<br />
complications<br />
• Expensive<br />
• Cannot be done<br />
without C arm facility
Acticon Neosphincter<br />
• Modification of urinary<br />
sphincter 3 parts:<br />
1) inflatable cuff<br />
around anus<br />
2) central pump (labia<br />
in Fe; scrotum in M)<br />
3) regulating balloon<br />
in Space of Retzius
Consider for:<br />
Artificial Bowel Sphincter<br />
• 30 % failed SNS<br />
• Congenital<br />
malformation<br />
• Absent sphincters<br />
• Significant loss of<br />
tissue due to injury
• N=52 1996-2010<br />
• F/U 64 +/- 46.5 mos<br />
Results of ABS<br />
• 26 (50%) required revision (most due to<br />
microperforation)<br />
• 14 (26.9%) definitive explantation (43% due to<br />
infection)<br />
• 35 with active device: fecal incontinence score<br />
(p
Artificial Sphincter: Complications<br />
• Range from 23-67%<br />
• Infection/perineal wound problems<br />
• Mechanical failure<br />
• Difficult evacuation<br />
• Still about 30% after learning curve<br />
Wong 1996, Lehur 1997, Vaizey 1998,<br />
Savoye 2000, Lehur 2002, O’Brien 2004
Change in <strong>Fecal</strong> <strong>Incontinence</strong> with ABS:<br />
Lehur<br />
1998<br />
Altomare<br />
2001<br />
Devasa<br />
2002<br />
O’Brien<br />
2004<br />
Using Wexner Score<br />
n preop postop % change<br />
13 17 4.5 74%<br />
28 14.9 2.6 83%<br />
53 17 4.0 74%<br />
14 19 4.8 89%
Antegrade Colonic Enema (ACE)<br />
• 1990 Malone<br />
– for children with neurogenic<br />
disorders<br />
• Continent conduit for intermittent<br />
catheterization<br />
– Appendix/ cecum/ ileum/<br />
descending colon<br />
• Irrigation of the colon and rapid and<br />
controlled large bowel purging<br />
• Does not preclude other future surgery
Antegrade Continence Enema<br />
• 10 adults F/U 17 mos; 80%<br />
significant reduction in FI<br />
episodes<br />
Malone 1990; Krogh 1998
<strong>Fecal</strong> <strong>Incontinence</strong>: Stoma<br />
• For patients who have failed<br />
or are not candidates for<br />
other surgical repairs<br />
• Old treatment, but can be<br />
done via a minimally<br />
invasive approach<br />
• Allows opportunity to leave<br />
home, attend work, and<br />
social functions
<strong>Fecal</strong> <strong>Incontinence</strong>: Future<br />
Magnetic anal encirclement Mesh sling of anus
Posterior Tibial Nerve Stimulation<br />
• First work for FI from Shafik<br />
in 2003 (Eur Surg Res)<br />
• Last 7 yr 7 other studies, all<br />
from Europe total 129 pts<br />
• All failed conservative tx<br />
• Heterogenecity in study pts,<br />
methodology, and outcomes<br />
Findlay et al Int J Colorectal Dis 2011;<br />
Leroi et al Am J Gastroenterol 2012
Posterior Tibial Nerve Stimulation<br />
• All tx protocols vary duration,<br />
timing, electrical frequency<br />
but all utilize portable external<br />
pulse generator<br />
• Current to post tib nerve<br />
proximal to medial malleolus<br />
with needle or adhesive<br />
electrode<br />
Findlay et al Int J Colorectal Dis 2011
Posterior Tibial Nerve Stimulation<br />
PTNS protocols:<br />
• Alt day 20 Hz for 30 min<br />
• Daily 10 Hz for 20 min<br />
• Weekly 20 Hz for 30 min<br />
• Twice wk 20 Hz for 30 min<br />
• Twice day ?? Hz for 20 min<br />
Findlay et al Int J Colorectal Dis 2011
90<br />
80<br />
70<br />
60<br />
50<br />
40<br />
30<br />
20<br />
10<br />
0<br />
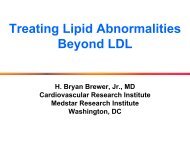
Shafik<br />
'03 n=32<br />
Summary PTNS trials<br />
achievement of primary endpoint<br />
Queralto<br />
'06 n=10<br />
Mentes<br />
'07 n=2<br />
Vitton<br />
'09 n=12<br />
De la<br />
Portilla<br />
'09 n=16<br />
Govaert<br />
'09 n=22<br />
Boyle<br />
'10 n=31<br />
Findlay<br />
'10 n=13
<strong>Fecal</strong> <strong>Incontinence</strong>: Treatment<br />
• Optimal treatment regime may<br />
be complex and tailored<br />
combination of various surgical<br />
and non-surgical treatment