Ph D Thesis - "Gr.T. Popa" Iasi
Ph D Thesis - "Gr.T. Popa" Iasi
Ph D Thesis - "Gr.T. Popa" Iasi

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
University of Medicine and <strong>Ph</strong>armacy „<strong>Gr</strong>. T. Popa” Iaşi<br />
Dental Medicine <strong>Ph</strong>aculty<br />
<strong>Ph</strong>armacology Department<br />
Head of Department: Prof. <strong>Ph</strong>D. Mihai Nechifor<br />
Variations of plasma and saliva<br />
concentration of some bivalent cations in<br />
pattients with oro-maxillo-facial area<br />
pathology and their pharmacological<br />
influences<br />
Scientific coordinator,<br />
Prof. phD. Mihai Nechifor<br />
<strong>Ph</strong> D <strong>Thesis</strong><br />
IAŞI<br />
– 2010 –<br />
<strong>Ph</strong>D Student,<br />
Assit. Prof., MD, Elena Luca<br />
1
General plan of the thesis<br />
<strong>Thesis</strong> Synopsis<br />
Introduction. Aims. Motivation for thesis theme election.<br />
CURENT KNOWLEDGE STAGE IN THE FIELD<br />
Chapter I<br />
The role of bivalent cations in the human body and in the oro-maxillo-facial<br />
area<br />
I. Calcium<br />
I. 1. Distribution in the human body<br />
I. 2. Recommended daily intake and natural sources<br />
I. 3. Elements of pharmacokinetics<br />
I. 4. Roles in the human body<br />
I. 5. Misbalances – pathology involvements<br />
I. 6. <strong>Ph</strong>armacotherapy uses<br />
II.. Magnezium<br />
II. 1. Distribution in the human body<br />
II. 2. Recommended daily intake and natural sources<br />
II. 3. Elements of pharmacokinetics<br />
II. 4. Roles in the human body<br />
II. 5. Misbalances – pathology involvements<br />
II. 6. <strong>Ph</strong>armacotherapy uses<br />
III. Iron<br />
III. 1. Distribution in the human body<br />
III. 2. Recommended daily intake and natural sources<br />
III. 3. Elements of pharmacokinetics<br />
III. 4. Roles in the human body<br />
III. 5. Misbalances – pathology involvements<br />
III. 6. <strong>Ph</strong>armacotherapy uses<br />
IV. Zinc<br />
IV. 1. Distribution in the human body<br />
IV. 2. Recommended daily intake and natural sources<br />
IV. 3. Elements of pharmacokinetics<br />
IV. 4. Roles in the human body<br />
IV. 5. Misbalances – pathology involvements<br />
IV. 6. <strong>Ph</strong>armacotherapy uses<br />
V. Copper<br />
V. 1. Distribution in the human body<br />
V. 2. Recommended daily intake and natural sources<br />
V. 3. Elements of pharmacokinetics<br />
V. 4. Roles in the human body<br />
V. 5. Misbalances – pathology involvements<br />
V. 6. <strong>Ph</strong>armacotherapy uses<br />
Chapter II<br />
Main pathology groups of in the oro-maxillo-facial area<br />
Chapter III<br />
Main groups of therapeutic drugs used in the oro-maxillo-facial area<br />
pathology<br />
2
OWN CONTRIBUTIONS<br />
Chapter I<br />
Technics and methods used for the determinations of metallic ions<br />
concentrations in biological fluids and tissues<br />
Chapter II<br />
Technics and methods udes for data statistical interpretation<br />
Chapter III<br />
Patients selection<br />
Chapter IV<br />
Sampling and primary prelucration of sampled biologic material (blood and<br />
saliva) in patients and volunteers, in order to determine the concentration of<br />
bivalent cations calcium, magnesium, iron, zinc, and copper<br />
Chapter V<br />
Research on variation of serum and saliva concentrations of some bivalent<br />
cations (Ca 2+ , Mg 2+ , Fe 2+ , Zn 2+ , Cu 2+ ) suppurations of the oro-maxillo-facial area<br />
I. Introduction<br />
II. Aims<br />
III. Subjects and method<br />
IV. Results<br />
V. Discutions<br />
VI. Conclusion<br />
Chapter VI<br />
Research on variation of serum and saliva concentrations of some bivalent<br />
cations (Ca 2+ , Mg 2+ , Fe 2+ , Zn 2+ , Cu 2+ ) chronic odontogenic maxillary sinusitis<br />
I. Introduction<br />
II. Aims<br />
III. Subjects and method<br />
IV. Results<br />
V. Discutions<br />
VI. Conclusion<br />
Chapter VII<br />
Research on variation of serum and saliva concentrations of some bivalent<br />
cations (Ca 2+ , Mg 2+ , Fe 2+ , Zn 2+ , Cu 2+ ) malignant tumours of the oro-maxillo-facial<br />
area<br />
I. Introduction<br />
II. Aims<br />
III. Subjects and method<br />
IV. Results<br />
V. Discutions<br />
VI. Conclusion<br />
Chapter VIII<br />
Research on variation of serum and saliva concentrations of some bivalent<br />
cations (Ca 2+ , Mg 2+ , Fe 2+ , Zn 2+ , Cu 2+ ) benignant tumours of the oro-maxillo-facial<br />
area<br />
I. Introduction<br />
II. Aims<br />
III. Subjects and method<br />
IV. Results<br />
V. Discutions<br />
VI. Conclusion<br />
Chapter IX<br />
3
Research on variation of serum and saliva concentrations of some bivalent<br />
cations (Ca 2+ , Mg 2+ , Fe 2+ , Zn 2+ , Cu 2+ ) fractures of the oro-maxillo-facial area<br />
I. Introduction<br />
II. Aims<br />
III. Subjects and method<br />
IV. Results<br />
V. Discutions<br />
FINAL CONCLUSIONS<br />
REFERENCES<br />
<strong>Ph</strong> D <strong>Thesis</strong> Synopsis<br />
I. Introduction. and motivation for thesis theme election.<br />
Bivalent cations (Ca 2+ , Mg 2+ , Zn 2+ , Cu 2+ , Mn 2+ etc) play important roles in the<br />
whole human and animal body.<br />
Misbalances in intra and extra-cellular concentrations of these cations are involved<br />
in the pathogenic mechamisms of numerous diseases.<br />
The tough elements of the dento-maxillar apparatus, calcium and magnesium are<br />
found in high concentrations. Calcium represent 37.9% of the enamel elements and<br />
25.9% of dentin elements, while the maxilla bone contains 22.5% calcium. Magnesium<br />
represents 0.42% of the enamel elements, 0.82% of dentin elements and 0.26% of<br />
maxilla bone elements (Hallsworth A. S. et al., 1972). Manganese concentration is<br />
higher in enamel than in dentin. Manganese concentration reaches its peak at the age of<br />
approximately 12 in both genders, than it slowly decreases with aging. Thus, manganese<br />
concentration in enamel was found to be 7.4±0.13 ppm at 10-12 years of age and it<br />
decreases to 6.67±0.12 at the age of 25.<br />
Appart from the structural role, which is particularely important for calcium and<br />
magnesium, the mentioned ions, either macro-elements or trace elements, exercite<br />
important functional roles, for example glandular secretion (saliva formation and<br />
excretion is dependent on both calcium and zinc ions) (Liu X. et al., 2007). (Goto T. et<br />
al., 2008). Zinc is found in secretory granules in the salivary gland. Zinc, together with<br />
many zinc-dependent enzymes, is closely involved in the saliva production and<br />
secretion, as well as in the contraction of the myoepithelial cells in the salivary glands.<br />
There are about 300 zinc-dependent enzymes and other few hundreds are<br />
magnesium-dependent for their activity. Zinc homeostasis is also important for the<br />
protection against salivarz calculi formation. In subgingival calculus, zinc concentration<br />
was found to be 5.4 times higher than in supragingival calculus. Homeostazia zincului<br />
la nivel seric şi salivar are, rol în protecţia contra formării calculilor supragingivali<br />
(Knuutilla M. et al., 1981; Knuutilla M. et al., 1979). Copper stimulates the activity of<br />
dental osteoclasts.<br />
Oral cavity tissues present a series of characteristics, some of which being<br />
mentioned above:<br />
- the permanent contact of the oral mucosa with both blood and saliva;<br />
- direct contact with nor only to breath air, but also with food and ingested liquids;<br />
- there are exposed to important mechanical solicitations during mastication;<br />
- the presence of microbial commensal flora.<br />
It also important to notice that different materials used in medical dental practice<br />
contain important quantities of bivalent cations, mentioning that zinc oxide and calcium<br />
hydroxide represent some of the most frequently used such materials.<br />
4
Misbalances in the concentrations of numerous substances in the blood, including<br />
cations, is also reflected in case of salivary concentrations, saliva being a very easy to<br />
sample biological fluid.<br />
Zinc deficiency, as well as the decreased zinc vs. copper concentrations ratio, has<br />
been identified as a risk factor for the development of lots of infections, with different<br />
localizing and etiological agent, as it determines immunity impairment. Yinc, as well as<br />
copper, limits the adhesion of Porphyromonas gingivalis (but not Streptococcus oralis)<br />
to periodontal structures, by favoring proteins adhesion to bacterial cell surface. The<br />
fact could be speculated for prevention of periodontal disease, underlining the role of<br />
different bivalent cations in the development of periodontal disease and generally in oral<br />
infections (Tamura M. and Ochiai K., 2009). Zinc deficiency is also accompanied by<br />
taste disturbances, salivary secretion disturbances, burning mouth syndrome.<br />
Zinc deficiency, as well as decreased zinc vs. copper concentrations ratio, is also<br />
considered a risk factor for malignant tumors development. In case of different types of<br />
cancers, including oral cavity cancers, zinc concentration, al well as ratio between zinc<br />
and copper serum concentration, is decreased. Oral neoplasm represent about 1 – 1.5%<br />
of cancers developed in the human body. Considering the antagonism between copper<br />
and zinc, including intestinal absorption antagonism, it is considered that zinc vs.<br />
copper concentrations ratio is more important than concentration of yinc and copper<br />
taken separately.<br />
Several systemic diseases influence salivary concentration in different bivalent<br />
cations. In this context, it has been showed that saliva from patients suffering from<br />
diabetes mellitus, calcium concentration is significantly increased, while Zn 2+ and Mg 2+<br />
concentrations are significantly decreased vs. normal gender and age match-controls.<br />
In chronic rheumatoid arthritis in children, zinc salivary level is decreased<br />
compared to normal age-paired controls (Una M. et al., 2004).<br />
Also, bivalent cations are found in tooth constituting-elements, misbalances in<br />
their concentrations being involved in tooth pathology. Magnesium is found in a greater<br />
concentration in dentin compared to enamel (Hallsworth AS. et al., 1972).<br />
A series of level found in tooth (and not only) such as hexokinase, are dependent<br />
on magnesium for their proper activity. There are data suggesting that increased<br />
magnesium tooth level is associated with increased carbohydrates consumption and may<br />
be involved in tooth decay apparition. Okazaki M. et al., 2007, considers that both<br />
magnesium and carbohydrates increase the solubility of apatite crystals and favours<br />
tooth decay. By annualizing the composition of carietic milk teeth in comparison with<br />
teeth without caries, Niedzielska K et al., 1990, found that carietic teeth contain more<br />
manganese and copper, but less zinc compared to normal ones.<br />
It is important to notice that both the individual cationic concentrations and the<br />
ratio between their concentrations are important. Different cations concentration in teeth<br />
is both age and gender-dependent and also the way their misbalances are involved in<br />
teeth pathology is different at different ages.<br />
Increased concentration of Mg 2+ in serum or other fluids was associated with<br />
malignant tumours development (Varazashvili V.L.M. et al., 2006).<br />
It is important to notice that both the individual cationic concentrations and the<br />
ratio between their concentrations are important. Different cations concentration in<br />
teeth is both age and gender-dependent and also the way their misbalances are involved<br />
in teeth pathology is different at different ages.<br />
II. The aim of this study is to investigate possible changes in the concentrations<br />
of serum and saliva bivalent cations (Ca 2+ , Mg 2+ , Zn 2+ , Fe 2+ , Cu 2 ) in patients with<br />
different pathology of the oro-maxillo-facial area:<br />
5
- infections (suppurations of the oro-maxillo-facial area and chronic odontogenic<br />
maxillary sinusitis);<br />
- tumours oro-maxillo-facial area (both malignant and benignant);<br />
- fractures of the oro-maxillo-facial area.<br />
III. Patients and method. The studied group consisted in adult (minimum age<br />
18) patients hospitalised in the oro-maxillo-facial clinic of “Sfântul Spiridon” Hospital<br />
Iaşi, hospitalised between 2006 and 2008. Studies were performed in the conditions of<br />
obtaining the necessary ethical authorisations and included patients have given their<br />
informed consent.<br />
The exclusion criteria for patients with suppurations of the oro-maxillo-facial<br />
area, chronic odontogenic maxillary sinusitis benignant tumours of the oro-maxillofacial<br />
area and fractures of the oro-maxillo-facial area, as well as for the corresponding<br />
control group are the following:<br />
• chronic diseases (diabetes mellitus, collagenoses, alcoholism, arterial<br />
hypertension, cardiac failure, chronic or acute allergic diseases, chronic obstructive<br />
pulmonary disease, liver cirrhosis, liver insufficiency, kidney failure, chronic allergic<br />
diseases);<br />
• patients to which medication containing Ca 2+ , Mg 2+ , Fe 2+ , Zn 2+ , Cu 2+ has<br />
been administered within 2 weeks prior to recruiting, no matter the route;<br />
• infectious pathology of any kind, either acute or chronic;<br />
• acute allergic diseases;<br />
• administration of diuretic medication within 2 weeks prior to recruiting, no<br />
matter the route;<br />
• administration of medication which modifies absorption, transport,<br />
distribution, metabolism, elimination or balance of the studied cations within 2 weeks<br />
prior to recruiting, no matter the route;<br />
• pregnant or breastfeeding women;<br />
• dehydrated or over-hydrated persons;<br />
• malabsorption, malnutrition, diarrhoea or digestive transit impairment;<br />
• surgical interventions within 6 weeks prior to the study;<br />
• active bleeding into the oral cavity;<br />
• malignant tumours, no matter the localisation;<br />
• bone fractures 6 weeks prior to the study )apart from the main diagnosis in<br />
case of fractures studied group);<br />
• metallic prosthetic materials (any kind, any localisation).<br />
In case of malignant tumours group, the presence of different pathologic<br />
conditioned imposed that patients with arterial hypertension, collagenoses, infections,<br />
either acute or chronic, allergic pathology, chronic obstructive pulmonary disease were<br />
also included. A correspondent gender and age matched controlled, with similar<br />
pathology, have been assigned as comparing controls for this group, being addes to the<br />
control group used as reference to patients with suppurations of the oro-maxillo-facial<br />
area, chronic odontogenic maxillary sinusitis benignant tumours of the oro-maxillofacial<br />
area and fractures of the oro-maxillo-facial area.<br />
Blood and saliva samples were collected before any therapeutic intervention or<br />
diagnosis procedure, 12 hours after the last meal, between 7 00 and 9 00 A. M..<br />
Blood samples were collected in biochemistry test-tubes with clotting accelerator<br />
and centrifuges, within no more than 30 minutes after sampling, for 10 minutes at 4000<br />
rotations per minute. Serum was separated and kept at -20ºC in simple test-tubes until<br />
determination.<br />
6
Saliva samples were collected by asking the volunteer to chew a cotton pad in the<br />
form of a cylinder for 5 minutes. The pad was then introduced in a tube and<br />
centrifuged. The supernatant was separated and kept at -20ºC in simple test-tubes until<br />
determination.<br />
Serum and salivary concentration of the studied cations (Ca 2+ , Mg 2+ , Zn 2+ , Fe 2+ ,<br />
Cu 2 ) was performed by atomic absorption spectrofotometry. We have also assessed for<br />
serum and saliva Ca 2+ /Mg 2+ and Zn 2+ / Cu 2+ concentrations ratio.<br />
Data were statistically interpreted with ANOVA.<br />
Number of volunteers<br />
50<br />
45<br />
40<br />
35<br />
30<br />
25<br />
20<br />
15<br />
10<br />
5<br />
0<br />
7<br />
9<br />
7<br />
2<br />
12<br />
Control group 1<br />
5 4 5<br />
18 - 34 35 - 49 50 - 64 > 65 Total<br />
9<br />
Age (years)<br />
Women Men Total<br />
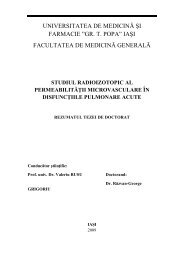
Fig. 1. Age and sex distribution diagram for control group 1 (reference for<br />
patients diagnosed with suppurations of the oro-maxillo-facial area, chronic<br />
odontogenic maxillary sinusitis benignant tumours of the oro-maxillo-facial area and<br />
fractures of the oro-maxillo-facial area).<br />
Number of volunteers<br />
80<br />
70<br />
60<br />
50<br />
40<br />
30<br />
20<br />
10<br />
0<br />
Control group 2<br />
17 17<br />
7<br />
2<br />
9 9 8<br />
7<br />
10<br />
18 - 34 35 - 49 50 - 64 > 65 Total<br />
Age (years)<br />
Women Men Total<br />
Fig. 2. Age and sex distribution diagram for control group 2 (reference for<br />
patients diagnosed with malignant tumours of the oro-maxillo-facial area).<br />
6<br />
11<br />
7<br />
13<br />
13<br />
24<br />
24<br />
34<br />
19<br />
33<br />
43<br />
67<br />
7
Number of volunteers<br />
50<br />
45<br />
40<br />
35<br />
30<br />
25<br />
20<br />
15<br />
10<br />
5<br />
0<br />
Suppurations group<br />
13 13<br />
8<br />
10<br />
7 6 7 6 7<br />
2<br />
4<br />
18 - 34 35 - 49 50 - 64 > 65 Total<br />
Age (years)<br />
Women Men Total<br />
Fig. 3. Age and sex distribution diagram for control diagnosed with suppurations<br />
of the oro-maxillo-facial area.<br />
Number of volunteers<br />
25<br />
20<br />
15<br />
10<br />
5<br />
0<br />
4<br />
2<br />
6<br />
Chronic odontogenic maxillary sinusitis group<br />
7<br />
4<br />
3 3<br />
2<br />
11<br />
5 5<br />
3<br />
2<br />
18 - 34 35 - 49 50 - 64 > 65 Total<br />
Age (years)<br />
Women Men Total<br />
Fig. 4. Age and sex distribution diagram for group 1 diagnosed with chronic<br />
odontogenic maxillary sinusitis.<br />
Number of volunteers<br />
70<br />
60<br />
50<br />
40<br />
30<br />
20<br />
10<br />
0<br />
Malignant tumours group<br />
18<br />
15<br />
11<br />
6 8 7 8<br />
7 7<br />
2<br />
18 - 34 35 - 49 50 - 64 > 65 Total<br />
Age (years)<br />
Women Men Total<br />
16<br />
23<br />
26<br />
12<br />
27<br />
21<br />
11<br />
37<br />
47<br />
23<br />
64<br />
8
Fig. 5. Age and sex distribution diagram for group diagnosed with malignant<br />
tumours of the oro-maxillo-facial area.<br />
Number of volunteers<br />
25<br />
20<br />
15<br />
10<br />
5<br />
0<br />
1<br />
2<br />
3<br />
5<br />
Benignant tumours group<br />
8<br />
3 3 3<br />
3<br />
18 - 34 35 - 49 50 - 64 > 65 Total<br />
6<br />
Age (years)<br />
Women Men Total<br />
Fig. 6. Age and sex distribution diagram for group diagnosed with benignant<br />
tumours of the oro-maxillo-facial area.<br />
Number of volunteers<br />
70<br />
60<br />
50<br />
40<br />
30<br />
20<br />
10<br />
0<br />
Fractures group<br />
15 17 15<br />
11 12 11 9<br />
4 5 4 3<br />
18 - 34 35 - 49 50 - 64 > 65 Total<br />
Age (years)<br />
Women Men Total<br />
Fig. 7. Age and sex distribution diagram for group diagnosed with fractures of<br />
the oro-maxillo-facial area.<br />
IV. Results.<br />
1. In case of patients with suppurations of the oro-maxillo-facial area,<br />
compared to control healthy volunteers group, our study had found:<br />
decreased serum zinc concentration (0.98±0.17 mg/L vs. 1.08±0.19mg/L,<br />
p
increased saliva magnesium concentration (3.76±0.39 mg/L vs.<br />
3.57±0.41mg/L, p
Fig. 10. Ratio between serum calcium concentration and serum magnesium<br />
concentration in healthy control volunteers and in patients with suppurations of the oromaxillo-facial<br />
area.<br />
2<br />
1,5<br />
1<br />
0,5<br />
0<br />
Ratio between serum zinc and copper<br />
concentration<br />
1,32±0,18<br />
**<br />
0,89±0,02<br />
Control group<br />
Patients with suppurations of the oro-maxillo-facial area<br />
Fig. 11. Ratio between serum zinc concentration and serum copper concentration<br />
in healthy control volunteers and in patients with suppurations of the oro-maxillo-facial<br />
area.<br />
mg / L<br />
5<br />
4<br />
3<br />
2<br />
1<br />
0<br />
Saliva magnesium concentration<br />
3,57±0,41<br />
*<br />
3,76±0,39<br />
Control group<br />
Patients with suppurations of the oro-maxillo-facial area<br />
Fig. 12. Magnesium saliva concentration in healthy control volunteers and in<br />
patients with suppurations of the oro-maxillo-facial area.<br />
20<br />
15<br />
10<br />
5<br />
0<br />
Ratio between saliva calcium and magnesium<br />
concentration<br />
15,45±2,42<br />
*<br />
14.53±2,41<br />
Control group<br />
Patients with suppurations of the oro-maxillo-facial area<br />
11
Fig. 13. Ratio between saliva calcium concentration and saliva magnesium<br />
concentration in healthy control volunteers and in patients with suppurations of the oromaxillo-facial<br />
area.<br />
Mg 2+ - saliva concentration (mg / L)<br />
5<br />
4,8<br />
4,6<br />
4,4<br />
4,2<br />
4<br />
3,8<br />
3,6<br />
3,4<br />
3,2<br />
y = 0,1413x + 0,2568<br />
R 2 = 0,5196<br />
Correlation between serum and saliva magnesium in patients<br />
3<br />
20 22 24 26 28 30 32<br />
Mg 2+ - serum concentration (mg / L)<br />
Fig. 14. Correlation between serum and saliva magnesium in healthy control<br />
volunteers and in patients with suppurations of the oro-maxillo-facial area.<br />
Apart from iron serum concentration, which is lower in women (p
mg / L<br />
30<br />
25<br />
20<br />
15<br />
10<br />
5<br />
0<br />
Magnesium serum concentration<br />
23,81±2,47<br />
**<br />
25,26±1,76<br />
Control group<br />
Patients with chronic odontogenic maxillary sinusitis<br />
Fig. 15. Magnesium serum concentration in healthy control volunteers and in<br />
patients with chronic odontogenic maxillary sinusitis.<br />
mg / L<br />
1,20<br />
1,00<br />
0,80<br />
0,60<br />
0,40<br />
0,20<br />
0,00<br />
Iron serum concentration<br />
0,85±0,15<br />
*<br />
0,78±0,13<br />
Control group<br />
Patients with chronic odontogenic maxillary sinusitis<br />
Fig. 16. Iron serum concentration in healthy control volunteers and in patients<br />
with chronic odontogenic maxillary sinusitis.<br />
mg / L<br />
1,00<br />
0,80<br />
0,60<br />
0,40<br />
0,20<br />
0,00<br />
Magnesium serum concentration<br />
WOMEN<br />
0,81±0,09<br />
**<br />
0,71±0,08<br />
Control group<br />
Patients with chronic odontogenic maxillary sinusitis<br />
Fig. 17. Iron serum concentration in healthy control volunteers women and in<br />
women with chronic odontogenic maxillary sinusitis.<br />
13
mg / L<br />
1,5<br />
1<br />
0,5<br />
0<br />
Zinc serum concentration<br />
1,08±0,19<br />
**<br />
0,95,19±0,17<br />
Control group<br />
Patients with chronic odontogenic maxillary sinusitis<br />
Fig. 18. Zinc serum concentration in healthy control volunteers and in patients<br />
with chronic odontogenic maxillary sinusitis.<br />
mg / L<br />
5<br />
4<br />
3<br />
2<br />
1<br />
0<br />
Magnesium saliva concentration<br />
3,57±0,41<br />
*<br />
3,76±0,38<br />
Control group<br />
Patients with chronic odontogenic maxillary sinusitis<br />
Fig. 19. Magnesium saliva concentration in healthy control volunteers and in<br />
patients with chronic odontogenic maxillary sinusitis.<br />
mg / L<br />
0,4<br />
0,3<br />
0,2<br />
0,1<br />
0<br />
Iron saliva concentration<br />
0,30±0,04<br />
*<br />
0.28±0,07<br />
Control group<br />
Patients with chronic odontogenic maxillary sinusitis<br />
Fig. 20. Iron saliva concentration in healthy control volunteers and in patients with<br />
chronic odontogenic maxillary sinusitis.<br />
14
20<br />
10<br />
0<br />
Ratio between saliva calcium and magnesium<br />
concentration<br />
Control group<br />
15,45±2,42<br />
*<br />
14,38±2,01<br />
Patients with suppurations chronic odontogenic maxillary<br />
sinusitis<br />
Fig. 21. Ratio between saliva calcium concentration and saliva magnesium<br />
concentration in healthy control volunteers and in patients with chronic odontogenic<br />
maxillary sinusitis.<br />
Mg 2+ - saliva concentration (mg / L)<br />
5,00<br />
4,80<br />
4,60<br />
4,40<br />
4,20<br />
4,00<br />
3,80<br />
3,60<br />
3,40<br />
3,20<br />
Correlation between serum and saliva magnesium in patients<br />
y = 0,1319x + 0,4322<br />
R 2 = 0,3678<br />
3,00<br />
20,00 21,00 22,00 23,00 24,00 25,00 26,00 27,00 28,00 29,00 30,00<br />
Mg 2+ - serum concentration (mg / L)<br />
Fig. 22. Correlations between serum and saliva magnesium concentration in<br />
healthy control volunteers and in patients with chronic odontogenic maxillary sinusitis .<br />
Apart from iron serum concentration, which is lower in women (p
decreased serum zinc mass concentration versus serum copper mass<br />
concentration ratio (1.20±0.40 vs. 1.37±0.48, p
mg / L<br />
1,00<br />
0,50<br />
0,00<br />
Control group<br />
Magnesium serum concentraion<br />
WOMEN<br />
0,79±0,08<br />
**<br />
0,74±0,10<br />
Patients with malignant tumours of the oro-maxillo-facial area<br />
Fig. 25. Iron serum concentration in control volunteers (women) and in patients<br />
with malignant tumours of the oro-maxillo-facial area (women).<br />
mg / L<br />
1,5<br />
1<br />
0,5<br />
0<br />
Zinc serum concentraion<br />
1,05±0,17<br />
*<br />
1,00±0,18<br />
Control group<br />
Patients with malignant tumours of the oro-maxillo-facial area<br />
Fig. 26. Zinc serum concentration in control volunteers and in patients with<br />
malignant tumours of the oro-maxillo-facial area.<br />
mg / L<br />
1,2<br />
1<br />
0,8<br />
0,6<br />
0,4<br />
0,2<br />
0<br />
Copper serum concentraion<br />
0,82±0,18<br />
*<br />
0,88±0,21<br />
Control group<br />
Patients with malignant tumours of the oro-maxillo-facial area<br />
Fig. 27. Coper serum concentration in control volunteers and in patients with<br />
malignant tumours of the oro-maxillo-facial area.<br />
17
2<br />
1,5<br />
1<br />
0,5<br />
0<br />
Ratio between serum zinc and copper<br />
concentration<br />
1,37±0,48<br />
*<br />
1,20±0,40<br />
Control group<br />
Patients with malignant tumours of the oro-maxillo-facial area<br />
Fig. 28. Ratio between saliva zinc concentration and copper magnesium<br />
concentration in healthy control volunteers and in patients with malignant tumours of<br />
the oro-maxillo-facial area.<br />
mg / L<br />
5<br />
4<br />
3<br />
2<br />
1<br />
0<br />
Magnesium saliva concentration<br />
3,61±0,37<br />
*<br />
3,73±0,40<br />
Control group<br />
Patients with malignant tumours of the oro-maxillo-facial area<br />
Fig. 29. Magnesium saliva concentration in control volunteers and in patients with<br />
malignant tumours of the oro-maxillo-facial area.<br />
mg / L<br />
0,8<br />
0,6<br />
0,4<br />
0,2<br />
0<br />
Copper saliva concentration<br />
0,61±0,07<br />
*<br />
0,63±0,06<br />
Control group<br />
Patients with malignant tumours of the oro-maxillo-facial area<br />
Fig. 30. Copper saliva concentration in control volunteers and in patients with<br />
malignant tumours of the oro-maxillo-facial area.<br />
18
Cu 2+ - saliva concentration<br />
(mg / L)<br />
0,8<br />
0,75<br />
0,7<br />
0,65<br />
0,6<br />
0,55<br />
0,5<br />
0,45<br />
0,4<br />
Correlation between serum and saliva magnesium in<br />
patients y = 0,151x + 0,4638<br />
R 2 = 0,4189<br />
0,4 0,6 0,8 1 1,2 1,4 1,6 1,8<br />
Cu 2+ - serum concentration (mg / L)<br />
Fig. 31. Correlations between serum and saliva copper concentration in healthy<br />
control volunteers and in patients with malignant tumours of the oro-maxillo-facial area.<br />
Apart from iron serum concentration, which is lower in women (p
Some of the most evident signs liked to zinc deficiency are related to immune<br />
system function impairment. As a result of immunodeficiency, the susceptibliity to viral<br />
infectins, especially to viral infections, is increased. Zinc deficiency determines thymus<br />
involution, impairment of delayed immune response, decreased T-cells in peripheral<br />
blood, decreased proliferative response of T-cells to phytohemagglutinin, inhibition of<br />
T-helper lymphocytes and natural-killer cells activity, as well as neutrophils functions<br />
and antibodies (Walravens P. A. et al., 1979). Zinc deficiency is also associated with<br />
decreased between T-helper 1 vs. T-helper 2 and decreased IFNγ production. From the<br />
molecular point of view, apoptosis of T-cells line precursors is influenced by zinc ions<br />
by expressions of Bcl-2/Bax genes, as zinc inhibits 3, 6, 7, and 8 caspases. In mature T<br />
lymphocytes, zinc is necessary for stimulation of some enzymes such as C-proteinkinase<br />
and tirosin-kinase C in the lymphocytes (LkC) (Hönscheid A. et al., 2009).<br />
In both patients with oro-maxillo-facial area suppurative infections and patients<br />
with chronic odontogenic maxillary sinusitis, decreases zinc serum level compared to<br />
healthy volunteers controls (p
proven to be beneficial, as it normalizes the activity of cyclooxygenase-2 and reduces<br />
cell proliferation rate.<br />
Numerous other studies have identified changes in zinc, copper, or zinc vs. copper<br />
concentration in serum, tissue or other biological fluids in patients with malignant<br />
tumors:<br />
o Varghese I. et al., 1987 have shown decreased Zn 2+ concentration, decreased<br />
Cu 2+ concentration and decreased ration Zn 2+ /Cu 2+ in serum, in patients with<br />
premalignant and malignant lesions of the oral cavity;<br />
o Gupta S. K. et al., 2005 have shown decreased Zn 2+ , increased Cu 2+ and<br />
decreased ration Zn 2+ /Cu 2+ in serum , in patients with carcinoma of the gallbladder;<br />
o Błoniarz J. et al., 2003 a have shown decreased Zn 2+ , increased Cu 2+ in saliva<br />
in patients with oral cancers;<br />
o Akçil E. et al., 2004 have shown decreased plasma zinc concentration<br />
(p
showed that Mg-dependent ATP-ase is involved in the development of some<br />
microorganisms capable of invading the salivary glands. It is possible that increased<br />
ratio between serum magnesium and calcium represents a predisposition factor to<br />
bacterial suppurations of oro-maxillo-facial area. Moreover, magnesium is also<br />
responsible for the expression of some Salmonella enterica genes (Lejona S. et al.,<br />
2003).<br />
There are also important data suggesting that magnesium excess is linked to<br />
immune suppression:<br />
Increased dietary magnesium intake suppreses some immune system functions<br />
(decreases mytogenic response of lymphocytes to lipopolysaccharide, decreases<br />
production of reactive oxygen species level by macrophages and nitrogen monoxide<br />
production) (Son E. W. et al., 2007);<br />
The intensity of inflammatory reaction, as non-specific immune response of<br />
the body, is also impaired in case of increased extra-cell magnesium concentration<br />
(Mazur A. et al., 2007).<br />
In our study, both serum and saliva magnesium concentration was found increased<br />
in patients with malignant tumors of the oro-maxillo-facial. The result is concordant<br />
with some other researcher’s findings:<br />
• Shpitzer T. et al., 2007, showed increased Mg 2+ saliva concentrations in<br />
patients with oral carcinomas;<br />
• Błoniarz J. et al., 2003, showed increased serum and saliva Mg 2+<br />
concentrations, in patients with oral carcinomas;<br />
• <strong>Gr</strong>ădinaru I. et al., 2008 showed increased serum and saliva Mg 2+<br />
concentrations, in patients with parotid gland malignant tumors, II – III;<br />
On the othe hand, Akçil E. et al., 2004 showed that there are no changes in<br />
erythrocytes magnesium levels in laryngeal malignant tumors groups compared to<br />
healthy volunteers.<br />
There are also authors suggesting that magnesium deficiency may be a state<br />
predisposing to malignant tumors development, as magnesium deficiency determines<br />
endothelium and fibroblastic replicative senescence; Mildred et al., 1993 shows that in a<br />
synthesis study referring to magnesium dietary deficiency and malignant tumors<br />
development, but does not neglect apparently paradox data suggesting the contrarium.<br />
Also, our research has revealed that, also there are no changes in saliva iron<br />
concentration; there is a significant decrease in serum iron concentration in women with<br />
malignant tumors of the oro-maxillo-facial area. However, we have not performed a<br />
hematological complete evaluation for correlations indexes. We consider the finding<br />
due to association of tumor anemia.<br />
Błoniarz J. et al., 2003 shows increased saliva iron concentration in patients with<br />
oral cancers, whreas serum iron is not chanced in patients with squamos carcinomas.<br />
VI. Conclusions<br />
1. In case of oro-maxillo-facial area suppurations, a moderate, but significant<br />
increase in saliva magnesium concentration, as well as in magnesium vs. calcium<br />
concentrations ratio in saliva has been determined, together with decreased serum zinc<br />
concentration; these elements may be considered a marker for the development of a oral<br />
suppuration;<br />
2. There are no significant differences in the saliva and serum concentrations of<br />
Ca 2+ , Mg 2+ , Zn 2+ , Fe 2+ and Cu 2+ in patients with fractures of the oro-maxillo-facial<br />
territory;<br />
22
3. There are no significant differences in the saliva and serum concentrations of<br />
Ca 2+ , Mg 2+ , Zn 2+ , Fe 2+ and Cu 2+ in patients with benignant tumours of the oro-maxillofacial<br />
area;<br />
4. In case of patients with malignant tumours of the oro-maxillo-facial area, zinc<br />
serum concentration is slightly, but significantly decreased, while saliva magnesium<br />
concentration is slightly, but significantly increased;<br />
5. In case of patients with chronic odontogenic maxillary sinusitis, serum and<br />
saliva magnesium concentration is slightly, bust statistically significant, increased.<br />
It may be possible that the ration between salivary calcium and magnesium<br />
concentration, correlated with zinc serum decrease are involved in the development of<br />
different pathological states of the oro-maxillo-facial area.<br />
References<br />
1. Akçil E, Caylakli F, Akiner M, Koçak M. Trace element concentrations and<br />
superoxide dismutase and catalase activities in benign and malignant larynx tumors.<br />
Biol Trace Elem Res. 2004; 101: 193-201<br />
2. Alarcón OM, Burguera JL, Burguera M, Suárez N, Reinosa J. Changes in<br />
copper, zinc and iron content in serum and saliva in various otorhinolaryngological<br />
ailments. J Trace Elem Electrolytes Health Dis. 1989; 3: 203-8<br />
3. Bales CW, Freeland-<strong>Gr</strong>aves JH, Askey S, Behmardi F, Pobocik RS, Fickel<br />
JJ, <strong>Gr</strong>eenlee P. Zinc, magnesium, copper, and protein concentrations in human saliva:<br />
age- and sex-related differences. Am J Clin Nutr. 1990; 51: 462-9<br />
4. Balkan ME, Ozgüneş H. Serum protein and zinc levels in patients with<br />
thoracic empyema. Biol Trace Elem Res. 1996; 54: 105-112<br />
5. Błoniarz J, Rahnama M, Zareba S, Swiatkowski W. The influence of<br />
carcinogenesis in the oral cavity on the level of zinc, copper and iron in serum. Rocz<br />
Panstw Zakl Hig. 2004; 55: 235-241<br />
6. Błoniarz J, Rahnama M, Zareba S. Influence of carcinogenesis in the oral<br />
cavity on the level of some bioelements in the saliva. Rocz Panstw Zakl Hig. 2003; 54:<br />
295-300<br />
7. Cardoso SV, Silveira-Júnior JB, De Carvalho Machado V, De-Paula AM,<br />
Loyola AM, De Aguiar MC. Expression of metallothionein and p53 antigens are<br />
correlated in oral squamous cell carcinoma. Anticancer Res. 2009; 29: 1189-1193.<br />
8. Dass CL, Walsh MF, Seo S, Shiratsuchi H, Craig DH, Basson MD. Irrigant<br />
divalent cation concentrations influence bacterial adhesion. J Surg Res. 2009; 156: 57-<br />
63<br />
9. Enwonwu CO, Falkler WA Jr, Idigbe EO, Afolabi BM, Ibrahim M,<br />
Onwujekwe D, Savage O, Meeks VI. Pathogenesis of cancrum oris (noma):<br />
confounding interactions of malnutrition with infection. Am J Trop Med Hyg. 1999; 60:<br />
223-32<br />
10. Fong LY, Jiang Y, Riley M, Liu X, Smalley KJ, Guttridge DC, Farber JL.<br />
Prevention of upper aerodigestive tract cancer in zinc-deficient rodents: inefficacy of<br />
genetic or pharmacological disruption of COX-2. Int J Cancer. 2008; 122: 978-989<br />
11. Fong LY, Zhang L, Jiang Y, Farber JL. Dietary zinc modulation of COX-2<br />
expression and lingual and esophageal carcinogenesis in rats. J Natl Cancer Inst. 2005;<br />
97: 40-50<br />
12. Fonseca FV, Fonseca de Souza AL, Mariano AC, Entringer PF, Gondim<br />
KC, Meyer-Fernandes JR. Trypanosoma rangeli: characterization of a Mg-dependent<br />
ecto ATP-diphosphohydrolase activity. Exp Parasitol. 2006; 112: 76-84<br />
23
13. Goto T, Shirakawa H, Furukawa Y, Komai M. Decreased expression of<br />
carbonic anhydrase isozyme II, rather than of isozyme VI, in submandibular glands in<br />
long-term zinc-deficient rats. Br J Nutr. 2008; 99: 248-53<br />
14. <strong>Gr</strong>ădinaru I, Ghiciuc CM, Popescu E, Nechifor C, Mândreci I, Nechifor M.<br />
Blood plasma and saliva levels of magnesium and other bivalent cations in patients<br />
with parotid gland tumors. Magnes Res. 2007; 20: 254-258<br />
15. <strong>Gr</strong>ant WB. An ecological study of cancer mortality rates including indices for<br />
dietary iron and zinc. Anticancer Res. 2008; 28: 1955-1963<br />
16. Gupta SK, Singh SP, Shukla VK. Copper, zinc, and Cu/Zn ratio in carcinoma<br />
of the gallbladder. J Surg Oncol. 2005; 91: 204-208<br />
17. Hallsworth AS, Robinson C, Weatherbell JA. Mineral and magnesium<br />
distribution within the approximal carious lesion of dental enamel. Caries Res. 1972; 6:<br />
156-168<br />
18. Hönscheid A, Rink L, Haase H. T-lymphocytes: a target for stimulatory and<br />
inhibitory effects of zinc ions. Endocr Metab Immune Disord Drug Targets. 2009; 9:<br />
132-144<br />
19. Knuuttila M, Lappalainen R, Kontturi-Närhi V. Concentrations of Ca, Mg,<br />
Mn, Sr and Zn in supra- and subgingival calculus. Scand J Dent Res. 1979; 87: 192-196<br />
20. Knuuttila M, Lappalainen R, Lammi S. Zn concentration of human<br />
subgingival calculus related to F, Mg and Cu contents. Scand J Dent Res. 1981; 89:412-<br />
6<br />
21. Lejona S, Aguirre A, Cabeza ML, García Véscovi E, Soncini FC. Molecular<br />
characterization of the Mg2+-responsive <strong>Ph</strong>oP-<strong>Ph</strong>oQ regulon in Salmonella enterica. J<br />
Bacteriol. 2003; 185: 6287-6294<br />
22. Liu X, Cheng KT, Bandyopadhyay BC, Pani B, Dietrich A, Paria BC,<br />
Swaim WD, Beech D, Yildrim E, Singh BB, Birnbaumer L, Ambudkar IS.<br />
Attenuation of store-operated Ca2+ current impairs salivary gland fluid secretion in<br />
TRPC1(-/-) mice. Proc Natl Acad Sci U S A. 2007 30; 104:17542-7<br />
23. Mazur A, Maier JA, Rock E, Gueux E, Nowacki W, Rayssiguier Y.<br />
Magnesium and the inflammatory response: potential physiopathological implications.<br />
Arch Biochem Biophys. 2007; 458: 48-56<br />
24. Niedzielska K, Struzak-Wysokińska M, Wujec Z. Analysis of correlations<br />
between the content of various elements in hard tissues of milk teeth with and without<br />
caries. Czas Stomatol. 1990; 43: 316-322<br />
25. Shpitzer T, Bahar G, Feinmesser R, Nagler RM. A comprehensive salivary<br />
analysis for oral cancer diagnosis. J Cancer Res Clin Oncol. 2007; 133: 613-7<br />
26. Son EW, Lee SR, Choi HS, Koo HJ, Huh JE, Kim MH, Pyo S. Effects of<br />
supplementation with higher levels of manganese and magnesium on immune function.<br />
Arch <strong>Ph</strong>arm Res. 2007; 30: 743-9<br />
27. Sutherland S. Several therapies may prevent or reduce the severity of oral<br />
mucositis associated with cancer treatment. Evid Based Dent. 2006; 7: 104-105<br />
28. Tamura M, Ochiai K. Zinc and copper play a role in coaggregation inhibiting<br />
action of Porphyromonas gingivalis. Oral Microbiol Immunol. 2009; 24: 56-63<br />
29. Turnlund JR, Keen CL, Smith RG. Copper status and urinary and salivary<br />
copper in young men at three levels of dietary copper. Am J Clin Nutr. 1990; 51: 658-<br />
664<br />
30. Una M, Tamer L, Pata YS, Kilies S, Dec Germenic U, Akbas Y, Serum<br />
levels of antioxidant vitamins copper and magnesium in patients with chronic<br />
rheumatoid arthritis, J. Trace Elem and Electrol Med Biol, 2004; 18: 189-192<br />
31. Unal M, Tamer L, Pata YS, Kilic S, Degirmenci U, Akbaş Y, Görür K, Atik<br />
U. Serum levels of antioxidant vitamins, copper, zinc and magnesium in children with<br />
chronic rhinosinusitis. J Trace Elem Med Biol. 2004; 18: 189-92<br />
24
32. Varazashvili L, Osmanova V, Giorgobiani L, Tushishvili D. Study of zinc<br />
content in blood serum of the patients with malignant tumors of the digestive systems.<br />
Georgian Med News. 2006; 137: 19-21<br />
33. Varghese I, Sugathan CK, Balasubramoniyan G, Vijayakumar T. Serum<br />
copper and zinc levels in premalignant and malignant lesions of the oral cavity.<br />
Oncology. 1987; 44: 224-227<br />
34. Walravens PA. Zinc metabolism and its implications in clinical medicine. West<br />
J Med. 1979; 130: 133-142<br />
25