Small Vessel Vasculitis
Small Vessel Vasculitis
Small Vessel Vasculitis

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Small</strong> <strong>Vessel</strong> <strong>Vasculitis</strong><br />
Banff- Rocky Mountain<br />
Barry Kassen, MD, FRCPC,FACP<br />
Head, Division of Internal Medicine – UBC/VGH/SPH<br />
Acting Head, Division of Community Internal Medicine<br />
November, 2009
<strong>Small</strong> <strong>Vessel</strong> <strong>Vasculitis</strong><br />
Objectives<br />
1. To understand small vessel vasculitis<br />
2. To understand an approach to therapy of small<br />
vessel vasculitis
<strong>Small</strong> <strong>Vessel</strong> <strong>Vasculitis</strong><br />
Classification of <strong>Vasculitis</strong><br />
1. Large vessel vasculitis<br />
2. Medium vessel vasculitis<br />
3. <strong>Small</strong> vessel vasculitis<br />
Plus: Antineutrophil Cytoplasmic Antibodies (ANCA)
<strong>Small</strong> <strong>Vessel</strong> <strong>Vasculitis</strong><br />
Classification (continued)<br />
Large <strong>Vessel</strong> <strong>Vasculitis</strong><br />
Takayasu’s<br />
Giant Cell Arteritis<br />
2. Medium Sized <strong>Vessel</strong> <strong>Vasculitis</strong><br />
Polyarteritis Nodosa (PAN)<br />
Microscopic Polyarteritis (MPA)<br />
Kawasaki’s Disease<br />
Primary Central Nervous System <strong>Vasculitis</strong><br />
3. <strong>Small</strong> <strong>Vessel</strong> <strong>Vasculitis</strong><br />
Churg-Strauss Arteritis (CSA)<br />
Wegeners Granulomatosis (WG)<br />
Microscopic Polyarteritis (MPA)<br />
Henoch- Schonlein Purpura<br />
Essential Cryoglobulinemic <strong>Vasculitis</strong><br />
Hypersensitivity <strong>Vasculitis</strong><br />
<strong>Vasculitis</strong> Secondary to Connective Tissue Disorders<br />
<strong>Vasculitis</strong> Secondary to Viral Infections
<strong>Small</strong> <strong>Vessel</strong> <strong>Vasculitis</strong><br />
Mimics and Secondary Causes of <strong>Vasculitis</strong><br />
Mimics of vasculitis Secondary causes of vasculitis<br />
Atheroembolic disease Infections Tuberculosis<br />
Atheromatous vascular disease Hepatitis B<br />
Anti-phospholipid syndrome Hepatitis C<br />
Multiple myeloma HIV<br />
Infective endocarditis Parvovirus<br />
Other chronic infections Cystic fibrosis<br />
Para-neoplastic syndromes Malignancy Lymphoma<br />
Autoinflammatory syndromes Solid organ malignancy<br />
Hypersensitivity reactions Connective tissue disorders Rheumatoid arthritis<br />
Cocaine and amphetamine abuse Systemic lupus erythematosus<br />
Scleroderma<br />
Sjogren’s syndrome<br />
Drugs Penicillamine<br />
Propylthiouracil<br />
Hydralazine<br />
Minocycline<br />
Cocaine<br />
Environmental exposure Dusts<br />
Silica
<strong>Small</strong> <strong>Vessel</strong> <strong>Vasculitis</strong><br />
A diagnostic pathway for vasculitis<br />
Components of a vasculitis diagnosis<br />
1. Compatible clinical phenotype<br />
2. Supported by specific serology (e.g. ANCA) or radiology (e.g.<br />
angiography)<br />
3. Confirmation by tissue biopsy<br />
4. Exclusion of mimics and secondary causes<br />
5. Observation over time to improve certainty of diagnosis<br />
(D. Jayne / Best Practice & Research Clinical Rheumatology 23 (2009) 445–453 447)
<strong>Small</strong> <strong>Vessel</strong> <strong>Vasculitis</strong><br />
Clinical Spectrum of Antineutrophil<br />
Cytoplasmic Antibodies (ANCA)<br />
1982- discovered<br />
Two types of ANCA assays<br />
Indirect Immunofluorescence assay (IF)<br />
Enzyme Linked Immunosorbent assay (ELISA)<br />
Target antigens<br />
Proteinase 3 (PR3)<br />
Myeloperoxidase (MPO)
<strong>Small</strong> <strong>Vessel</strong> <strong>Vasculitis</strong><br />
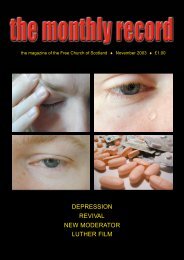
Immunofluorescence Patterns in <strong>Vasculitis</strong><br />
Incubate patients serum with ethanol-fixed neutrophils (alcohol fixed<br />
buffy coat leukocytes)<br />
2 patterns seen visually<br />
#1 C- ANCA<br />
There is diffuse straining throughout the cytoplasm. (antigen is<br />
proteinase 3)<br />
#2 P-ANCA<br />
There is staining around the nucleus (antigen is myeloperoxidase)<br />
Caution:<br />
ANCA testing has no references for normal range<br />
Positive predictive value for vasculitis 25%-50%<br />
There are other antigens in the cytoplasm (lactoferrin, elestase, etc.)<br />
ANA positive may give “false positive”. (to P-ANCA)
C-ANCA
P- ANCA
<strong>Small</strong> <strong>Vessel</strong> <strong>Vasculitis</strong><br />
Enzyme-Linked Immonoassays (ELISA)<br />
This test is more specific than I.F and so is performed following I.F.<br />
Antibodies to:<br />
• Proteinase 3 (PR3)<br />
• Myeloperoxidase (MPO)<br />
C-ANCA<br />
• Most cases antibody is to PR3<br />
P-ANCA<br />
• Most cases antibody to Myeloperoxidase (MPO)<br />
• ELISA has higher specificity and higher positive predicative<br />
values for vasculitis.
<strong>Small</strong> <strong>Vessel</strong> <strong>Vasculitis</strong><br />
Disease Associations with ANCA<br />
Wegener’s Granulomatosis, microscopic polyarteritis, Churg-Strauss, renal-limited<br />
vasculitis, drug induced vasculitis syndromes.<br />
Classic drug association is propylthiouracil or methimazole.<br />
Nonvasculitis Rheumatic Disorders<br />
RA, SLE, Sjogren’s Syndrome, JRA, Scleroderma<br />
Autoimmune Gastrointesinal Disorders<br />
Ulcerative Colitis<br />
Crohn’s disease<br />
Cystic Fribrosis<br />
Others: Subacute bacterial endocarditis<br />
Infectious mononucleosis<br />
graft vs.. host<br />
autoimmune hepatitis<br />
etc.
<strong>Small</strong> <strong>Vessel</strong> <strong>Vasculitis</strong><br />
ANCA<br />
Is a positive test a “True Positive” ?<br />
IF- positive predictive value for vasculitis- 45%<br />
ELISA- positive predictive value 83%<br />
IF plus ELISA-88%<br />
Does a negative ANCA exclude small vessel vasculitis?<br />
40% of limited Wegener’s are ANCA negative<br />
10% of severe Wegener’s are ANCA negative<br />
30% of MPA<br />
50% of CSS
<strong>Small</strong> <strong>Vessel</strong> <strong>Vasculitis</strong><br />
Does a positive ANCA alleviate the need for<br />
confirmation of diagnosis by tissue biopsy?<br />
The Predictive value of ANCA testing depends heavily on the clinical<br />
situation.<br />
Multi-centered European Collaborative study (Kidney International<br />
1998).<br />
Comparison of vasculitis patients with controls who had other<br />
vasculitis, other glomerulopathies, etc and 740 healthy<br />
volunteers.<br />
Sensitivity and specificity of ANCA (IF/ELISA) varied for WG,<br />
MPA, and pauci-immune vasculitis. Therefore a biopsy is still<br />
required in ANCA positive patients to make a diagnosis of<br />
Primary <strong>Vasculitis</strong>.
<strong>Small</strong> <strong>Vessel</strong> <strong>Vasculitis</strong><br />
Does a Rise in ANCA Predict a Disease Flare?<br />
WGET (Research group, 2005)<br />
180 patients followed by ANCA 3 monthly.<br />
No difference in median time to relapse, disease activity or organ<br />
involvement.<br />
Controversy, though, still exists.<br />
Does Persistently Negative ANCA Assure Disease<br />
quiescence?<br />
If initially positive then helpful for proof of remission.
<strong>Small</strong> <strong>Vessel</strong> <strong>Vasculitis</strong><br />
Epidemiology of <strong>Small</strong> <strong>Vessel</strong> <strong>Vasculitis</strong><br />
Is Systemic vasculitis becoming more common?<br />
Incidence of ANCA associated vasculitis in Norfolk, England<br />
1989-1993- incidence 20.3 case per million<br />
1999-2003- incidence 17.1 cases per million<br />
Incidence in Northern Germany<br />
1999-incidence 48 cases per million<br />
2002- incidence 42 cases per million
<strong>Small</strong> <strong>Vessel</strong> <strong>Vasculitis</strong><br />
Pathogenesis of <strong>Vasculitis</strong><br />
Do leukotriene inhibitors cause Churg-Strauss Syndrome?<br />
1998 Wechsler- 8 cases of glucocorticoid-dependant asthma treated with<br />
zafirlukast.<br />
Developed Eosinophilia, pulmonary infiltrates and cardiomyopathy.<br />
2003- Mayo Clinic Review (91 cases) of Churg-Strauss<br />
16 cases received leukotriene inhibitors before onset of disease.<br />
6 patients received leukotriene inhibitors during remission.<br />
4 years interval between onset of asthma and vasculitis in both groups (16/91;<br />
65/91)<br />
4/6 patients in remission received leukotrienes with no flare.
<strong>Small</strong> <strong>Vessel</strong> <strong>Vasculitis</strong><br />
What is the significance of ANCA among patients with<br />
Churg-Strauss <strong>Vasculitis</strong>?<br />
Patients with this disease may be ANCA (MPO) positive or negative.<br />
• Retrospective analysis 93 patients (1989-2004)<br />
• 35 ANCA Positive<br />
small vessel vasculitis disease<br />
Manifest by:<br />
Purpura (25.7% vs. 6.9%)<br />
• Pulmonary hemorrhage (20.0% vs. 0%)<br />
• Mononeuritic multiplex (51.4% vs. 24.1%)<br />
• Renal involvement (51.4% vs. 12.1%)<br />
• ANCA Negative Patients<br />
Parenchymal lung disease<br />
Cardiac involvement<br />
Are there 2 phenotypes based on ANCA status?<br />
ANCA positive with vasculitic manifestation?<br />
• ANCA negative with eosinophil driven processes leading to cardiopulmonary manifestation?
<strong>Small</strong> <strong>Vessel</strong> <strong>Vasculitis</strong><br />
Treatment of <strong>Vasculitis</strong><br />
Are short courses of cyclophosphamide effective for the treatment of<br />
ANCA associated vasculitis (AAV)?<br />
CYCAZAREM (Cyclophosphamide or Azathioprine as a Remission for <strong>Vasculitis</strong>)<br />
NEJM 2003.<br />
• Patients WG or MPA<br />
• Induction therapy: (3 months)<br />
Cyclophosphamide 2 mg/kg p.o.<br />
Prednisone 1 mg/kg/p/o.<br />
• Post induction: (3 month-12 months)<br />
Cyclophosphamide 1.5 mg/kg p.o.<br />
Azathioprine 2 mg/kg (prednisone 10 mg daily)<br />
• 12 months to 10 months all patients switched to AZA 1.5 mg/kg plus<br />
prednisone 7.5 mg daily.<br />
• Relapse rate the same:<br />
Cyclophosphamide- 14%<br />
AZA – 16%
<strong>Small</strong> <strong>Vessel</strong> <strong>Vasculitis</strong><br />
Is there a role for plasma exchange in the<br />
treatment of ANCA associated vasculitis?<br />
European union vasculitis study group (EUVAS) MEPEX Trial- 2007, 137 patients<br />
randomized to Methylprednisone IV or plasma exchange.<br />
Results:<br />
All patients had serum creatine greater than 500 micromoles<br />
Plasma exchange 7 over 2 weeks<br />
Methylprednisolone one gram daily x3<br />
Both groups received cyclophasphmade 2.5 mg/kg and prednisone 60 mg<br />
daily.<br />
35 died during the trial.<br />
23/35 died in the first 3months.<br />
71/137 had independent renal function.
<strong>Small</strong> <strong>Vessel</strong> <strong>Vasculitis</strong><br />
Mepex Trial Results (cont’d)<br />
Plasma exchange was associated with a significantly higher likelihood of being<br />
alive and having independent renal function at 3 months.<br />
69% in plasma exchange gp<br />
49% in methylprednisone gp<br />
Plasma exchange was associated with a significant reduction in risk of progression<br />
to end stage renal disease at one year.<br />
19% vs. 43%<br />
Mortality rate high in both groups 35/137 (infection, pulmonary hemorrhage, CVS)
<strong>Small</strong> <strong>Vessel</strong> <strong>Vasculitis</strong><br />
Are TNF inhibitors effective treatment of<br />
ANCA associated vasculitis?<br />
WGET (Wegener’s Granulomatosis etanercept trial)<br />
Design to see if etanercept, after induction therapy, would maintain<br />
remission ( in patients who were maintained on standard therapy)<br />
180 patients (follow up 27 months)<br />
50% patients who achieved remission 126/180 were able to<br />
maintain this.<br />
There was no difference in remission rate, flares or adverse events<br />
between groups.<br />
But, 6 etanercept patients developed malignancies (no control<br />
patients)
<strong>Small</strong> <strong>Vessel</strong> <strong>Vasculitis</strong><br />
Do early generalized ANCA associated vasculitis<br />
patients treated with methotrexate fare as well as<br />
those treated with cyclophosphamide ?<br />
NORAM (Non-renal Alternative with Methotrexate trial), De Grout- 2005.<br />
100 patients with limited Wegener’s received either methotrexate or<br />
cyclophosphamide with glucocortoids.<br />
6 month remission rates<br />
MTX-89.8%<br />
CYC- 93.5%<br />
18 month relapse rates<br />
MTX 69.5%<br />
CYC 46.5%<br />
Higher does of prednisone in MTX group 8.8 vs. 6.2
<strong>Small</strong> <strong>Vessel</strong> <strong>Vasculitis</strong><br />
Remission Maintenance in <strong>Vasculitis</strong><br />
When should remission maintenance be stopped for patients with<br />
ANCA associated vasculitis?<br />
NIH longitudal study (1992)<br />
33% cured after first course of RX.<br />
CYCAZAREM<br />
WG is more likely than MPA to flare.<br />
Clinical trials in AAV<br />
Support use of lose dose prednisone to maintain remission.
<strong>Small</strong> <strong>Vessel</strong> <strong>Vasculitis</strong><br />
Are patients with systemic vasculitis at risk of<br />
Venous thromboembolism?<br />
Venous obstruction (SVC or IVC occlusion) or Budd Chiari syndrome has<br />
been reported in Bechet’s disease.<br />
Superficial phlebitis…….. Buerger’s disease.<br />
Wegener’s Granulomatosis ……..venous thrombosis (Annals of Internal<br />
Med- 2005) is seven times greater than the incidence in patients with<br />
systemic lupus erythematosis.
<strong>Small</strong> <strong>Vessel</strong> <strong>Vasculitis</strong><br />
References<br />
<strong>Small</strong> vessel and Nuclear <strong>Vessel</strong> <strong>Vasculitis</strong>- Seo/Johnston, Arthritis and Rheumatism Vol 57, No.<br />
8, Dec 15, 2007, p 1552-1559.<br />
The Diagnosis of <strong>Vasculitis</strong>, Jayne, Best Practice and Research Clinical Rheumatology 23<br />
(2009) 445-453.<br />
EULAR Recommendations for the management of primary small and medium vessel vasculitis,<br />
Ann Rheum Dis 2009; 68; 310-317.<br />
The Last Classification of <strong>Vasculitis</strong>- Kallenberg, Clinic Rev Allerg Immunol (2008) 35:5-10<br />
Uptodate- 2009, Rhuematoid Disease Clinics of North America, <strong>Vasculitis</strong>- 2001<br />
Azathoprine or Methotrexate Maintenance for ANCA- Associated <strong>Vasculitis</strong>-Pagnoux, NEJM<br />
2008; 359; 2790-2803