Isolation of Legionella pneumophila from clinical & environmental ...
Isolation of Legionella pneumophila from clinical & environmental ...
Isolation of Legionella pneumophila from clinical & environmental ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
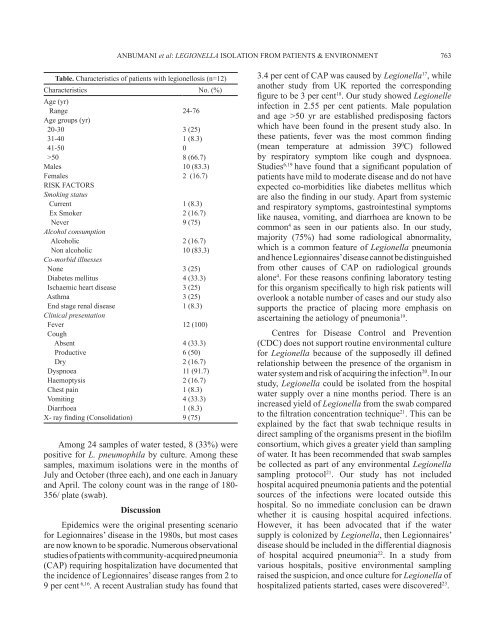
Table. Characteristics <strong>of</strong> patients with legionellosis (n=12)<br />
Characteristics No. (%)<br />
Age (yr)<br />
Range<br />
Age groups (yr)<br />
20-30<br />
31-40<br />
41-50<br />
>50<br />
Males<br />
Females<br />
RISK FACTORS<br />
Smoking status<br />
Current<br />
Ex Smoker<br />
Never<br />
Alcohol consumption<br />
Alcoholic<br />
Non alcoholic<br />
Co-morbid illnesses<br />
None<br />
Diabetes mellitus<br />
Ischaemic heart disease<br />
Asthma<br />
End stage renal disease<br />
Clinical presentation<br />
Fever<br />
Cough<br />
Absent<br />
Productive<br />
Dry<br />
Dyspnoea<br />
Haemoptysis<br />
Chest pain<br />
Vomiting<br />
Diarrhoea<br />
X- ray finding (Consolidation)<br />
ANBUMANI et al: LEGIONELLA ISOLATION FROM PATIENTS & ENVIRONMENT 763<br />
Among 24 samples <strong>of</strong> water tested, 8 (33%) were<br />
positive for L. <strong>pneumophila</strong> by culture. Among these<br />
samples, maximum isolations were in the months <strong>of</strong><br />
July and October (three each), and one each in January<br />
and April. The colony count was in the range <strong>of</strong> 180-<br />
356/ plate (swab).<br />
Discussion<br />
24-76<br />
3 (25)<br />
1 (8.3)<br />
0<br />
8 (66.7)<br />
10 (83.3)<br />
2 (16.7)<br />
1 (8.3)<br />
2 (16.7)<br />
9 (75)<br />
2 (16.7)<br />
10 (83.3)<br />
3 (25)<br />
4 (33.3)<br />
3 (25)<br />
3 (25)<br />
1 (8.3)<br />
12 (100)<br />
4 (33.3)<br />
6 (50)<br />
2 (16.7)<br />
11 (91.7)<br />
2 (16.7)<br />
1 (8.3)<br />
4 (33.3)<br />
1 (8.3)<br />
9 (75)<br />
Epidemics were the original presenting scenario<br />
for Legionnaires’ disease in the 1980s, but most cases<br />
are now known to be sporadic. Numerous observational<br />
studies <strong>of</strong> patients with community-acquired pneumonia<br />
(CAP) requiring hospitalization have documented that<br />
the incidence <strong>of</strong> Legionnaires’ disease ranges <strong>from</strong> 2 to<br />
9 per cent 6,16 . A recent Australian study has found that<br />
3.4 per cent <strong>of</strong> CAP was caused by <strong>Legionella</strong> 17 , while<br />
another study <strong>from</strong> UK reported the corresponding<br />
figure to be 3 per cent 18 . Our study showed Legionelle<br />
infection in 2.55 per cent patients. Male population<br />
and age >50 yr are established predisposing factors<br />
which have been found in the present study also. In<br />
these patients, fever was the most common finding<br />
(mean temperature at admission 39 0 C) followed<br />
by respiratory symptom like cough and dyspnoea.<br />
Studies 6,19 have found that a significant population <strong>of</strong><br />
patients have mild to moderate disease and do not have<br />
expected co-morbidities like diabetes mellitus which<br />
are also the finding in our study. Apart <strong>from</strong> systemic<br />
and respiratory symptoms, gastrointestinal symptoms<br />
like nausea, vomiting, and diarrhoea are known to be<br />
common 4 as seen in our patients also. In our study,<br />
majority (75%) had some radiological abnormality,<br />
which is a common feature <strong>of</strong> <strong>Legionella</strong> pneumonia<br />
and hence Legionnaires’ disease cannot be distinguished<br />
<strong>from</strong> other causes <strong>of</strong> CAP on radiological grounds<br />
alone 4 . For these reasons confining laboratory testing<br />
for this organism specifically to high risk patients will<br />
overlook a notable number <strong>of</strong> cases and our study also<br />
supports the practice <strong>of</strong> placing more emphasis on<br />
ascertaining the aetiology <strong>of</strong> pneumonia 19 .<br />
Centres for Disease Control and Prevention<br />
(CDC) does not support routine <strong>environmental</strong> culture<br />
for <strong>Legionella</strong> because <strong>of</strong> the supposedly ill defined<br />
relationship between the presence <strong>of</strong> the organism in<br />
water system and risk <strong>of</strong> acquiring the infection 20 . In our<br />
study, <strong>Legionella</strong> could be isolated <strong>from</strong> the hospital<br />
water supply over a nine months period. There is an<br />
increased yield <strong>of</strong> <strong>Legionella</strong> <strong>from</strong> the swab compared<br />
to the filtration concentration technique 21 . This can be<br />
explained by the fact that swab technique results in<br />
direct sampling <strong>of</strong> the organisms present in the bi<strong>of</strong>ilm<br />
consortium, which gives a greater yield than sampling<br />
<strong>of</strong> water. It has been recommended that swab samples<br />
be collected as part <strong>of</strong> any <strong>environmental</strong> <strong>Legionella</strong><br />
sampling protocol 21 . Our study has not included<br />
hospital acquired pneumonia patients and the potential<br />
sources <strong>of</strong> the infections were located outside this<br />
hospital. So no immediate conclusion can be drawn<br />
whether it is causing hospital acquired infections.<br />
However, it has been advocated that if the water<br />
supply is colonized by <strong>Legionella</strong>, then Legionnaires’<br />
disease should be included in the differential diagnosis<br />
<strong>of</strong> hospital acquired pneumonia 22 . In a study <strong>from</strong><br />
various hospitals, positive <strong>environmental</strong> sampling<br />
raised the suspicion, and once culture for <strong>Legionella</strong> <strong>of</strong><br />
hospitalized patients started, cases were discovered 23 .