Occupational Intakes of Radionuclides Part 1 - ICRP
Occupational Intakes of Radionuclides Part 1 - ICRP
Occupational Intakes of Radionuclides Part 1 - ICRP

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
983<br />
984<br />
985<br />
986<br />
987<br />
988<br />
989<br />
990<br />
991<br />
992<br />
993<br />
994<br />
995<br />
996<br />
997<br />
998<br />
999<br />
1000<br />
1001<br />
1002<br />
1003<br />
1004<br />
1005<br />
1006<br />
1007<br />
1008<br />
1009<br />
1010<br />
1011<br />
1012<br />
1013<br />
1014<br />
1015<br />
DRAFT REPORT FOR CONSULTATION<br />
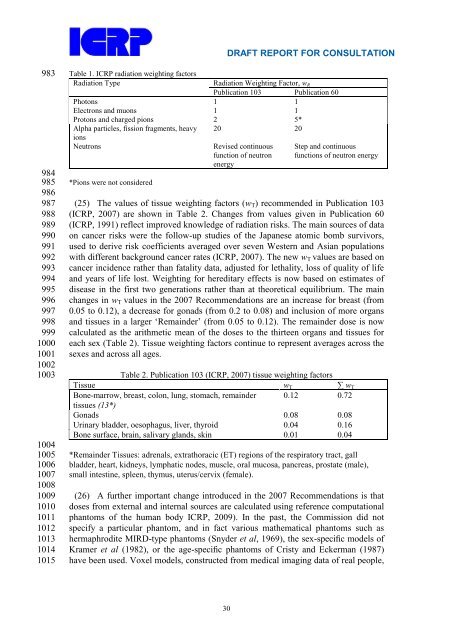
Table 1. <strong>ICRP</strong> radiation weighting factors<br />
Radiation Type Radiation Weighting Factor, wR<br />
Publication 103 Publication 60<br />
Photons 1 1<br />
Electrons and muons 1 1<br />
Protons and charged pions 2 5*<br />
Alpha particles, fission fragments, heavy<br />
ions<br />
20 20<br />
Neutrons Revised continuous Step and continuous<br />
function <strong>of</strong> neutron<br />
energy<br />
functions <strong>of</strong> neutron energy<br />
*Pions were not considered<br />
(25) The values <strong>of</strong> tissue weighting factors (wT) recommended in Publication 103<br />
(<strong>ICRP</strong>, 2007) are shown in Table 2. Changes from values given in Publication 60<br />
(<strong>ICRP</strong>, 1991) reflect improved knowledge <strong>of</strong> radiation risks. The main sources <strong>of</strong> data<br />
on cancer risks were the follow-up studies <strong>of</strong> the Japanese atomic bomb survivors,<br />
used to derive risk coefficients averaged over seven Western and Asian populations<br />
with different background cancer rates (<strong>ICRP</strong>, 2007). The new wT values are based on<br />
cancer incidence rather than fatality data, adjusted for lethality, loss <strong>of</strong> quality <strong>of</strong> life<br />
and years <strong>of</strong> life lost. Weighting for hereditary effects is now based on estimates <strong>of</strong><br />
disease in the first two generations rather than at theoretical equilibrium. The main<br />
changes in wT values in the 2007 Recommendations are an increase for breast (from<br />
0.05 to 0.12), a decrease for gonads (from 0.2 to 0.08) and inclusion <strong>of</strong> more organs<br />
and tissues in a larger ‘Remainder’ (from 0.05 to 0.12). The remainder dose is now<br />
calculated as the arithmetic mean <strong>of</strong> the doses to the thirteen organs and tissues for<br />
each sex (Table 2). Tissue weighting factors continue to represent averages across the<br />
sexes and across all ages.<br />
Tissue<br />
Table 2. Publication 103 (<strong>ICRP</strong>, 2007) tissue weighting factors<br />
wT ∑ wT<br />
Bone-marrow, breast, colon, lung, stomach, remainder<br />
tissues (13*)<br />
0.12 0.72<br />
Gonads 0.08 0.08<br />
Urinary bladder, oesophagus, liver, thyroid 0.04 0.16<br />
Bone surface, brain, salivary glands, skin 0.01 0.04<br />
*Remainder Tissues: adrenals, extrathoracic (ET) regions <strong>of</strong> the respiratory tract, gall<br />
bladder, heart, kidneys, lymphatic nodes, muscle, oral mucosa, pancreas, prostate (male),<br />
small intestine, spleen, thymus, uterus/cervix (female).<br />
(26) A further important change introduced in the 2007 Recommendations is that<br />
doses from external and internal sources are calculated using reference computational<br />
phantoms <strong>of</strong> the human body <strong>ICRP</strong>, 2009). In the past, the Commission did not<br />
specify a particular phantom, and in fact various mathematical phantoms such as<br />
hermaphrodite MIRD-type phantoms (Snyder et al, 1969), the sex-specific models <strong>of</strong><br />
Kramer et al (1982), or the age-specific phantoms <strong>of</strong> Cristy and Eckerman (1987)<br />
have been used. Voxel models, constructed from medical imaging data <strong>of</strong> real people,<br />
30