REVIEW OF LITERATURE ON DIGITAL MAMMOGRAPHY IN ...
REVIEW OF LITERATURE ON DIGITAL MAMMOGRAPHY IN ...
REVIEW OF LITERATURE ON DIGITAL MAMMOGRAPHY IN ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>REVIEW</strong> <strong>OF</strong> <strong>LITERATURE</strong> <strong>ON</strong> <strong>DIGITAL</strong><br />
<strong>MAMMOGRAPHY</strong> <strong>IN</strong> SCREEN<strong>IN</strong>G<br />
Prepared on behalf of the NHSBSP Digital Imaging<br />
Technologies Steering Group by K.C. Young and D. Kitou,<br />
National Coordinating Centre for the Physics of Mammography<br />
NHSBSP Equipment Report 0502<br />
December 2005
Enquiries<br />
Enquiries about this report should be addressed to:<br />
Dr K.C. Young<br />
National Coordinating Centre for the Physics of Mammography<br />
Regional Radiation Protection Service<br />
Royal Surrey County Hospital<br />
Guildford<br />
GU2 7XX<br />
Tel: 01483 406738<br />
Fax: 01483 406742<br />
Email: ken.young@nhs.net<br />
Published by<br />
NHS Cancer Screening Programmes<br />
Fulwood House<br />
Old Fulwood Road<br />
Sheffield<br />
S10 3TH<br />
Tel: 0114 271 1060<br />
Fax: 0114 271 1089<br />
Email: nhs.screening@cancerscreening.nhs.uk<br />
Website: www.cancerscreening.nhs.uk<br />
© NHS Cancer Screening Programmes 2005<br />
The contents of this document may be copied for use by staff working in the public sector but may<br />
not be copied for any other purpose without prior permission from the NHS Cancer Screening<br />
Programmes.<br />
The report is available in PDF format on the NHS Cancer Screening Programmes’ website<br />
Further copies<br />
Requests for further copies should be made to the Department of Health Publications Orderline,<br />
quoting NHSBSP Equipment Report 0502.<br />
Tel: 08701 555 455<br />
Fax: 01623 724 524<br />
Email: doh@prolog.uk.com<br />
Typeset by Prepress Projects Ltd, Perth (www.prepress-projects.co.uk)<br />
Printed by Duffield Printers
C<strong>ON</strong>TENTS<br />
Review of Literature on Digital Mammography in Screening<br />
NHSBSP December 2005 iii<br />
Page No<br />
1. <strong>IN</strong>TRODUCTI<strong>ON</strong> 1<br />
2. CL<strong>IN</strong>ICAL TRIALS 2<br />
2.1 Colorado Screening Trial I 2<br />
2.2 Colorado Screening Trial II 2<br />
2.3 Oslo I study 3<br />
2.4 Oslo II study 4<br />
2.5 ACR<strong>IN</strong>-DMIST Trial 5<br />
3. OTHER RESEARCH PUBLICATI<strong>ON</strong>S 7<br />
3.1 Microcalcification detection 7<br />
3.2 Image quality and lesion detection in clinical images 8<br />
3.3 Reasons for disagreement in interpretation of FFDM and SFM 9<br />
3.4 Other techniques in digital mammography 9<br />
4. C<strong>ON</strong>CLUSI<strong>ON</strong>S 12<br />
REFERENCES 13<br />
BIBLIOGRAPHY 15
Review of Literature on Digital Mammography in Screening<br />
NHSBSP December 2005 iv
. <strong>IN</strong>TRODUCTI<strong>ON</strong><br />
NHSBSP December 2005<br />
Review of Literature on Digital Mammography in Screening<br />
It is government strategy in the UK to implement both film-less and paper-less imaging departments by 2006. 1<br />
As a result, there is increasing pressure on and interest from breast screening programmes in moving to digital<br />
mammography. However, screen-film mammography is currently the only accepted imaging technique for<br />
screening, and any changes to the imaging technique should be made only following:<br />
• a review of the available evidence<br />
• consideration of the technical and clinical suitability of the equipment<br />
• assessment of the practical suitability for screening in the UK environment<br />
• assurance that the quality standards of the NHS Breast Screening Programme (NHSBSP) will, as a<br />
minimum, be maintained.<br />
At the beginning of 2005, the NHSBSP set up a steering group for digital mammography to address these<br />
issues. The steering group comprises representatives from the different professional groups and will oversee<br />
the evaluation and introduction of digital mammography for the breast screening programme. This report is<br />
a review of the current scientific literature on digital mammography and concentrates on its role in breast<br />
screening and the evidence for its clinical effectiveness. The five major publications on clinical trials are discussed<br />
in some detail in Chapter 2. Other types of research studies, such as phantom studies, are reported in<br />
Chapter 3. This chapter also reports briefly on the latest literature concerning the development of new imaging<br />
techniques using digital mammography, such as contrast enhancement and breast tomography. Apart from the<br />
major clinical trials, the review is not intended to be fully comprehensive. The proceedings of the biennial<br />
International Workshops on Digital Mammography provide numerous additional research papers that are not<br />
discussed individually here, but are listed in the bibliography.
Review of Literature on Digital Mammography in Screening<br />
2. CL<strong>IN</strong>ICAL TRIALS<br />
2. Colorado Screening Trial I<br />
The first results of a trial by Lewin et al 2 were published in 2001. This is referred to here as the Colorado<br />
Screening Trial I, and the main characteristics are summarised in Table 1. The study was performed with a<br />
screening population of 4945 women aged 40 years and older. The aim was to compare full field digital mammography<br />
(FFDM) with screen-film mammography (SFM) for cancer detection. Images were acquired using<br />
both modalities on each woman and were interpreted independently. Findings were evaluated with additional<br />
imaging and, if warranted, biopsy was performed. There were 152 biopsies resulting in the diagnosis of 35<br />
breast cancers. Twenty cancers were detected by SFM and 21 with FFDM. Four cancers were not detected by<br />
either modality but became palpable within a year and represented false negative findings with both modalities.<br />
Thus, no significant difference in the cancer detection rate was observed. FFDM had a significantly lower<br />
recall rate (11.5%) than SFM (13.8%).<br />
Comment: The main finding in this publication was the lack of a significant difference in cancer detection<br />
by SFM and FFDM. However, as the numbers of cancers detected were small, any difference would need to<br />
have been large in order to have been detected. It was also observed that a large proportion of cancers were<br />
detected using one modality but were not detected by the other. Thus, the sensitivity of each modality on its<br />
own seems very low by NHSBSP standards. The specificity of each modality was also low by UK standards<br />
with recall rates of 11–14%.<br />
2.2 Colorado Screening Trial II<br />
The second publication on the results of this trial reported an increase in the number of examinations to 6736<br />
and enabled an analysis of trends with time. 3 In addition, the reasons for the differences in interpretations<br />
between the two modalities were considered. In total, 6736 paired examinations were performed, with 1665<br />
subjects enrolling twice and 291 subjects enrolling three times with an interval of 11 months between examinations.<br />
Symptomatic patients were also imaged but were excluded from the analysis.<br />
The recall rate was 14.9% for SFM and 11.8% for FFDM, which was a significant difference (P < 0.001). The<br />
numbers of cancers detected by the two modalities are compared in Table 2. Eight cancers were not detected<br />
by either modality and were detected by palpation and biopsied within 12 months of the negative screening<br />
findings. These data indicate sensitivities of 66% (33/50) for SFM and 54% (27/50) for FFDM, but these<br />
were not significantly different. The authors indicate that such sensitivities are at or above the expected rate<br />
for their population.<br />
The reasons for cancers being detected by one modality and not the other were examined in detail. No dominant<br />
cause was found. Small differences in the superposition of tissue was one factor cited – and presumed<br />
to be due to slight variations in the projection or compression that were unrelated to the technology in use.<br />
Table Summary of study parameters: Colorado I<br />
Analogue system GE DMR x-ray set with Kodak Min-R 2000 film-screen system<br />
Digital system Prototype of the GE Senographe 2000D with soft copy reading<br />
Patient group Women attending for screening aged above 40<br />
Study type Paired examinations<br />
Number of women 4945<br />
Cancers detected by SFM 22<br />
Cancers detected by FFFM 21<br />
Total number of cancers detected 35<br />
NHSBSP December 2005 2
NHSBSP December 2005<br />
Review of Literature on Digital Mammography in Screening<br />
Table 2 Numbers of cancers with positive and negative screening results for the two modalities<br />
Positive on FFDM Negative on FFDM Totals<br />
Positive on SFM 18 15 33<br />
Negative on SFM 9 8 17<br />
Totals 27 23 50<br />
Differences in lesion conspicuity were also noticed between the modalities – in both directions. Human error<br />
and small differences in interpretation were also factors. The authors highlighted the significantly lower recall<br />
rate with FFDM. However, when they looked at the positive predictive value (PPV), this was similar at 3.3%<br />
(33/1001) for SFM and 3.4% (27/793) for FFDM.<br />
Comment: The main finding in this publication was the lack of a significant difference in cancer detection by<br />
SFM and FFDM. However, as the numbers of cancers were small, any difference would need to have been<br />
rather large in order to have been detected. The numbers of cancers detected by one modality but missed by the<br />
other seemed surprisingly large. One possible conclusion is that relatively subtle differences in presentation can<br />
affect the ability of film readers to detect cancers. It appears that slight variations in compression and view can<br />
mask cancers. This is something that needs to be borne in mind when comparing different modalities. In other<br />
words, it would be preferable to use the same compression and view. Many of the performance parameters (ie<br />
sensitivity, specificity, recall rate and PPV) were quite different from those found in the NHSBSP, suggesting<br />
that caution needs to be exercised in translating such US trial data to the UK context.<br />
2. Oslo I study<br />
In the first Oslo study, 3683 women between 50 and 69 years of age took part in a paired comparison of SFM<br />
and FFDM. 4 The study design is summarised in Table 3. Two standard views of each breast were acquired with<br />
FFDM with soft copy reading and SFM. A total of eight radiologists participated and were divided into two<br />
teams. The teams read the FFDM and SFM images in alternate weeks. The images were read independently<br />
by two radiologists with arbitration by a consensus meeting of the whole team. A five point rating scale was<br />
used for cancer probability, and recall rates, PPVs and cancer detection rates were determined. The mammograms<br />
from prior screening rounds were not offered at the screening interpretation but were available at<br />
consensus meetings. The results are summarised in Table 4, and show that there was no significant difference<br />
in cancer detection rate between the two modalities. The authors conducted a side-by-side analysis of cancer<br />
conspicuity and concluded that the two modalities were equal overall, although one modality or another led<br />
to greater conspicuity in specific cases.<br />
The authors concluded that cancers missed using FFDM (Table 5) were not due to a limitation in image quality<br />
as they were easily visible in retrospect. Rather, they believed that this may have been the result of a learning<br />
effect with the new FFDM soft copy reading environment. They also cited the use of a suboptimal reading<br />
environment (extraneous light sources) as a factor causing cancers to be missed using the FFDM system.<br />
Table Summary of study parameters: Oslo I<br />
Analogue x-ray set Siemens Mammomat 300 using 29 kV Mo/Mo<br />
Analogue film-screen Kodak Min-R 2000 film with Min-R 2190 screen<br />
Digital system GE Senographe 2000D in AOP mode<br />
Digital viewing modality Soft copy reading<br />
Patient group Women attending for repeat screening aged 50–69<br />
Study type Paired examinations<br />
Number of women 3683<br />
Total number of cancers detected 31 (detection rate = 0.84%)
Table Summary outcomes: Oslo I<br />
NHSBSP December 2005<br />
Review of Literature on Digital Mammography in Screening<br />
SFM FFDM P-value<br />
Recall rate 3.5% (128/3683) 4.6% (168/3683)<br />
Cancer detection rate 0.76% (28/3683) 0.62% (23/3683) 0.23<br />
PPV for recall on mammographic finding 20% (26/128) 12% (20/168)<br />
Table 5 Numbers of cancers with positive and negative screening results for the two modalities before consensus<br />
meeting<br />
Positive on FFDM Negative on FFDM Totals<br />
Positive on SFM 20 8 28<br />
Negative on SFM 3 – 3<br />
Totals 23 8 31<br />
Comment: The Oslo I study used screening methods quite similar to those used in the NHSBSP, and may<br />
therefore be more readily translated to the UK context than the Colorado studies. As in the Colorado studies,<br />
a number of cancers were missed by each modality, with FFDM tending to miss more (although FFDM and<br />
SFM were not significantly different in this regard). The importance of reader training and viewing conditions<br />
when using soft copy reading were emphasised by the authors, and these are issues that can be taken on<br />
board by the NHSBSP.<br />
2. Oslo II study<br />
The second Oslo study was not a continuation of the Oslo I study, but represented a new study that began five<br />
months after the first one finished. 5 In the Oslo I study, the women underwent both SFM and FFDM, ie it was<br />
a paired study. In the Oslo II study, women attending for screening were randomly allocated to either SFM<br />
or FFDM using the study parameters summarised in Table 6. A total of 25 263 women aged 45–69 attended.<br />
These women were divided into two groups: one for ages 45–49 and the other for ages 50–69. In each group,<br />
the women were randomised to undergo SFM (70%) or FFDM (30%). Two standard views of each breast<br />
were acquired, and independent double reading was performed using a five point rating scale for probability of<br />
cancer. Recall rates, PPVs and cancer detection rates were compared for the two age groups and modalities.<br />
The outcomes for the two age groups are shown in Tables 7 and 8. For both age groups combined, the detection<br />
rate was 0.41% (73/17911) for SFM and 0.59% (41/6997) for FFDM (P = 0.06). The difference in detection<br />
rates between SFM and FFDM was almost significant (P = 0.053) for the 50–69 age group. The recall rate<br />
for FFDM was significantly higher for the 50–69 age group. However, the effect of this appeared to result in<br />
greater cancer detection and similar PPV values for both modalities.<br />
Comment: As with the Oslo I study, the reading methods in the Oslo II study are similar to routine screening<br />
in the UK. Further evidence is provided that screening with FFDM in soft copy mode can yield similar cancer<br />
detection rates to SFM. Recall rates were slightly higher with FFDM, but at levels that would be acceptable<br />
in the NHSBSP. The authors pointed out that prior films were not available during this study, and that they<br />
might have improved the specificity. This study provides the best evidence that a production FFDM system<br />
can be used safely for screening. However, it should be borne in mind that this conclusion may be safely<br />
applied only to this specific model, and after the training and viewing condition issues raised in the Oslo I<br />
study have been addressed.
Review of Literature on Digital Mammography in Screening<br />
Table 6 Summary of study parameters: Oslo II<br />
Analogue x-ray set Siemens Mammomat 300 using 29 kV Mo/Mo<br />
Analogue film-screen Kodak Min-R 2000 film with Min-R 2190 screen<br />
Digital system GE Senographe 2000D in AOP mode<br />
Digital viewing modality Soft copy reading<br />
Patient groups Women attending for repeat screening aged 45–49<br />
Women attending for repeat screening aged 50–69<br />
Study type Randomised allocation SFM/FFDM split 70:30<br />
Number of women 25 263 (attended)<br />
Total number of cancers detected 120 (detection rate = 0.48%)<br />
Table 7 Summary outcomes: Oslo II, age 50–69<br />
SFM FFDM Significance<br />
Recall rate 2.5% (253/10 304) 3.8% (153/3985) P < 0.05<br />
Cancer detection rate 0.54% (56/10 304) 0.83% (33/3985) P = 0.053<br />
PPV for recall on mammographic finding 22.1% (56/253) 21.6% (33/153) NS<br />
NS, not significant.<br />
Table 8 Summary outcomes: Oslo II, age 45–49<br />
SFM FFDM P-value<br />
Recall rate 3.0% (231/7607) 3.7% (112/3012) NS<br />
Cancer detection rate 0.22% (17/7607) 0.27% (8/3012 NS<br />
PPV for recall on mammographic finding 7.4% (17/231) 7.1% (8/112) NS<br />
NS, not significant.<br />
2.5 ACR<strong>IN</strong>-DMIST Trial<br />
The American College of Radiology Information Network (ACR<strong>IN</strong>) conducted the Digital Mammography in<br />
Screening Trial (DMIST). 6,7 A total of 49 528 asymptomatic women were screened at 34 centres in the USA<br />
and Canada using the five types of digital equipment shown in Table 9. All women underwent both digital and<br />
screen-film mammography. Two standard views of each breast and any additional views required were taken<br />
with both systems. Each examination was interpreted independently by two separate readers and, depending<br />
on the findings of either study, a work-up was performed. The images were assessed by either hard or soft<br />
copy display depending on what was available with the system, as shown in Table 9. The scales that were<br />
used for the interpretation of the mammograms were a standard BI-RADS scale, probability of malignancy<br />
and a call back scale.<br />
The primary measurements of this study included area under the receiver operating characteristic (ROC) curve,<br />
sensitivity and specificity, PPV and negative predictive value (NPV). Secondary aims of the study are to assess<br />
the effects of patient characteristics such as age, lesion type and breast density on diagnostic accuracy. Finally,<br />
a direct and long term cost-effectiveness analysis of digital mammography is to be performed.<br />
The study showed no significant difference in the diagnostic accuracy between FFDM and SFM for the entire<br />
study population. However, the diagnostic accuracy of FFDM was significantly higher than SFM for three<br />
subgroups, as shown by the areas under the ROC curves in Table 10. The recall rates for SFM and FFDM were<br />
NHSBSP December 2005 5
Review of Literature on Digital Mammography in Screening<br />
both 8.5%. The sensitivities based on 455 days of follow up are shown in Table 11 and are relatively low for both<br />
methods. None of the differences in sensitivity reached a significant level. The authors also calculated higher<br />
sensitivities for a more usual 365 day follow up period. No evidence was found of a difference in diagnostic<br />
accuracy with the type of digital machine. Further publications, including a cost analysis, are promised.<br />
Comment: The DMIST trial is by far the largest clinical trial of digital mammography published to date. It<br />
provides strong evidence that, for the types of digital mammography evaluated, FFDM is no worse than SFM,<br />
and in fact has a significantly better diagnostic accuracy in women aged under 50 and in those with relatively<br />
dense breasts. The recall rate was rather higher and the sensitivities rather lower than would be expected in a<br />
European study. This seems to be the result of differences in the way that screening is carried out in the USA<br />
and Europe. However, the main conclusions could still apply to the UK context.<br />
Table 9 Imaging technique factors and display parameters of the digital systems used 6<br />
Machine<br />
Mean<br />
MGD<br />
type (mGy) Target/filter/kV Grid Soft copy display/monitors<br />
GE 2000D 1.7 Automated optimisation of Yes Two Siemens monitors (each<br />
parameters (Mo/Mo; Mo/Rh<br />
and Rh/Rh)<br />
2 k × 2.5 k)<br />
Fischer 1.8 W/Al/28–35 No: slot Two Barco monitors<br />
scan<br />
design<br />
(each 2 k × 2.5 k)<br />
NHSBSP December 2005 6<br />
Hard copy<br />
display<br />
Not applicable<br />
Kodak<br />
Dryview<br />
8600 or Agfa<br />
LR5200<br />
Fuji 5000MA 2.1 Mo/Mo/28 Yes Not applicable Fuji DryLaser<br />
FM/DPL<br />
Lorad/Trex 2.2 Mo/Mo/25–32 Yes Not applicable Agfa LR5200<br />
Lorad/<br />
Hologic<br />
MGD, mean glandular dose.<br />
2.5 Mo/Mo/25–32 Yes Two Barco monitors<br />
(each 2048 × 2560)<br />
Table 0 Summary of areas under the ROC curves in the DMIST trial<br />
Agfa LR5200<br />
Area under ROC curve<br />
Group (women) No of women SFM FFDM<br />
Significance<br />
All women 42 760 0.74 ± 0.02 0.78 ± 0.02 P = 0.18<br />
Women < 50 years 14 335 0.69 ± 0.05 0.84 ± 0.03 P = 0.002<br />
Women with dense breasts 19 897 0.68 ± 0.03 0.78 ± 0.03 P = 0.003<br />
Premenopausal or<br />
perimenopausal<br />
15 803 0.67 ± 0.05 0.82 ± 0.03 P = 0.002<br />
Table Sensitivities and specificities in the DMIST trial calculated using a 455 day follow up<br />
Sensitivity (± SE) Specificity (± SE)<br />
Group (women)<br />
SFM FFDM SFM FFDM<br />
All women 0.41 ± 0.03 0.41 ± 0.03 0.98 ± 0.001 0.98 ± 0.001<br />
Women < 50 years 0.35 ± 0.06 0.49 ± 0.06 0.98 ± 0.001 0.97 ± 0.001<br />
Women with dense breasts 0.36 ± 0.04 0.38 ± 0.04 0.98 ± 0.001 0.97 ± 0.001<br />
Premenopausal or perimenopausal 0.67 ± 0.05 0.82 ± 0.03 0.97 ± 0.001 0.97 ± 0.001
Review of Literature on Digital Mammography in Screening<br />
. OTHER RESEARCH PUBLICATI<strong>ON</strong>S<br />
3.1 Microcalcification detection<br />
3.1.1 Studies with patients<br />
Fischer et al 8 compared the sensitivity of FFDM and SFM in the detection of microcalcifications and evaluated<br />
their accuracy in microcalcification characterisation. Fifty-five patients with 57 microcalcification clusters<br />
were examined. For each cluster, a screen-film and a digital mammogram were obtained using a GE Senographe<br />
2000D digital system and a GE Senographe DMR with a Fuji UM-MA screen-film system. Evaluation<br />
criteria were image quality, the number of visible calcifications and the characterisation of the findings. For<br />
the characterisation, a five point BI-RADS scale was used where a score of 1 indicated no findings and a score<br />
of 5 was highly suggestive of malignancy. The sensitivity, specificity and image quality scores are shown in<br />
Table 12. The authors reported that FFDM generally detected more calcifications, but that the differences in<br />
specificity and sensitivity for malignant tumours were not significant.<br />
FFDM depicted a significantly higher number of microcalcifications than SFM. More specifically, the number<br />
of visible calcifications was the same for FFDM and SFM in 59% of the cases, whereas FFDM showed more<br />
calcifications in 41% of all cases. There was no case in which SFM showed more particles than FFDM. The<br />
authors concluded that the FFDM system with a 100 µm pixel size provides better image quality, a higher<br />
detection rate and more accurate characterisation of microcalcifications than SFM. 8<br />
Di Nubila et al 9 also investigated how the lower spatial resolution of an FFDM system affects microcalcification<br />
detection. Four radiologists examined the images of 52 surgical samples of non-palpable breast lesions<br />
with microcalcifications taken with both digital (GE Senographe 2000D) and analogue (GE Senographe<br />
DMR) modalities in standard and magnified view. The cases were classified into three groups depending on<br />
the number of microcalcifications in the surgical sample: fewer than 10, 10–30 and more than 30. The Kappa<br />
test was used to evaluate the differences in the numbers of microcalcifications shown in Table 13.<br />
The authors concluded that digital mammography was broadly similar to analogue imaging for standard<br />
views, but appeared to have an advantage when the magnification views were compared. Using a magnification<br />
technique allowed the detection of a larger number of microcalcifications than the standard technique,<br />
with either system.<br />
3.1.2 Studies with phantoms<br />
Rong et al 10 have imaged a phantom containing simulated microcalcifications of various sizes using four different<br />
systems: a flat panel (FP) system (ie as used in the GE Senographe 2000D), a small field-of-view charge<br />
coupled device (CCD) system, a high resolution computerised radiography (CR) system and a conventional<br />
screen-film (SFM) system. The phantom was created using 2 × 2 cm 2 Lucite squares containing simulated<br />
microcalcifications (calcium carbonate grains) at five possible locations. Three different microcalcification<br />
sizes were used ranging from about 120 µm to 160 µm, and three squares were created for each size; the resulting<br />
nine tiles were arranged into a 6 × 6 cm 2 phantom. Scores reflecting confidence ratings were given for all<br />
Table 2 Sensitivity and specificity for malignant tumours with microcalcifications by Fischer et al 8<br />
SFM FFDM<br />
Image quality (points) 3.36 4.25<br />
Sensitivity (%) 91.7 95.2<br />
Specificity (%) 39.3 41.4<br />
NHSBSP December 2005 7
Review of Literature on Digital Mammography in Screening<br />
Table Summary of microcalcification count 9<br />
Equal number of<br />
microcalcifications<br />
Larger number of<br />
microcalcifications<br />
Smaller number of<br />
microcalcifications<br />
Digital standard vs<br />
analogue standard<br />
No of<br />
cases %<br />
Digital magnification<br />
vs analogue<br />
magnification<br />
No of<br />
cases %<br />
images, and the results were used to determine the average confidence rating scores of the four systems. ROC<br />
analysis was also performed to assess and compare the detection accuracy of the systems. The areas under the<br />
ROC curves were significantly different, as shown in Table 14.<br />
The results showed that, using either the average confidence rating or ROC analysis, the FP system performed<br />
the best; second was the SFM system; the CCD system was third; and the CR system was last.<br />
Lai et al 11 also compared the ability of different systems to detect microcalcifications. The systems that<br />
were compared were a flat panel (FP), a CCD and a screen-film system using a phantom with simulated<br />
microcalcifications of various sizes (90–355 µm). The images were taken with two different backgrounds<br />
and two magnification modes. A slab of simulated 50% adipose and 50% glandular tissue was used for a<br />
uniform background and an anthropomorphic breast phantom for tissue structure background. To simulate<br />
the microcalcifications, calcium carbonate grains of various sizes were used. For the uniform background,<br />
the size ranged from 90 to 180 µm, and for the tissue structure background from 160 to 355 µm. A phantom<br />
for imaging was formed by two 2 × 2 cm 2 films, with five grains of the same size on each one placed in the<br />
2 × 2 mm 2 region. The FP and CCD images were printed on 8 × 10 inch films using a laser printer. Twelve<br />
viewers were asked to rate the visibility of each microcalcification using a five point scale, where a score of<br />
1 meant definitely not present and a score of 5 definitely present. Using a uniform background and no magnification,<br />
the FP system performed significantly better than the other two. With magnification, the SFM was<br />
similar to the FP, and both outperformed the CCD system. However, with tissue structure background and no<br />
magnification, the FP system was outperformed by the SFM and CCD. With magnification, the FP and CCD<br />
systems improved significantly, with the CCD outperforming both the SFM and FP. These results indicated<br />
that the performance of a mammography system depends not only on the detector technology used but also<br />
on the background structure and magnification.<br />
.2 Image quality and lesion detection in clinical images<br />
Obenauer et al 12 compared clinical FFDM (GE Senographe 2000D) and SFM images from the same patients<br />
using subjective comparisons of image quality and lesion detectability. Digital and conventional mammograms<br />
NHSBSP December 2005 8<br />
Analogue magnification<br />
vs analogue<br />
standard<br />
No of<br />
cases %<br />
Digital magnification<br />
vs digital standard<br />
No of<br />
cases %<br />
141 67.8 147 70.7 178 85.6 132 63.5<br />
37 17.8 52 25.0 24 11.5 62 29.8<br />
30 14.0 9 4.3 6 2.9 14 6.7<br />
Table Areas under the ROC curves for the four modalities<br />
Modality Area under ROC curve (A z ) Standard error in A z<br />
Flat panel 0.857 0.010<br />
Screen-film (SFM) 0.786 0.013<br />
CCD 0.756 0.013<br />
CR 0.683 0.015
Review of Literature on Digital Mammography in Screening<br />
were performed on 55 patients with cytologically or histologically proven tumours. Seventy-five digital mammograms<br />
of patients without tumours were also reviewed along with their screen-film mammograms taken 1.5<br />
years previously. Aspects such as contrast, exposure and the presence of artefacts were evaluated. A three-point<br />
ranking scale was used to judge different details such as the skin and other structures. The detectability and<br />
characterisation of microcalcifications and lesions were also compared and correlated to histology. 12 Artefacts<br />
were found in 78% of the conventional and in none of the digital mammograms. Some anatomical regions<br />
were better visualised by FFDM than by SFM. The authors concluded that digital mammography offers better<br />
image quality without artefacts and equal lesion detection. Lesion characterisation was found to be slightly<br />
better using FFDM even though differences in the final diagnostic decision were not significant.<br />
Fischmann et al 13 performed a study in which 200 women without visible or palpable breast lesions underwent<br />
digital mammography (GE Senographe 2000D) of one breast and SFM of the other. For all women, one<br />
breast was imaged with the FFDM system and the other with the SFM to avoid double radiation exposure<br />
of the breasts. The modalities were allocated randomly and the same compression was applied to both of the<br />
breasts and by the same radiographer. The imaging parameters were set automatically by both systems. Three<br />
readers independently evaluated image quality, visualisation of calcifications and masses under the same<br />
viewing conditions. There was no difference in the diagnostic classification of the microcalcifications, and<br />
also there were no significant differences in the detection of masses. Readers A and B found better contrast<br />
with FFDM in parenchymal tissue, whereas reader C found a better contrast in fatty tissue. All three readers<br />
found the breast parenchyma to be less dense with FFDM. Finally, in contrast to earlier studies, there was a<br />
non-significant tendency for a higher mean glandular dose with FFDM. Digital mammography demonstrated<br />
improved image quality with significantly better depiction of the nipple, skin and pectoral muscle and better<br />
microcalcification detection. 13<br />
Yamada et al 14 compared FFDM (GE Senographe 2000D) with SFM in a study of 24 patients undergoing<br />
surgery or biopsy, including 17 with carcinoma. Three readers evaluated hard copies of a total of 10 masses<br />
and 15 areas of microcalcification in terms of contrast, margin and type. FFDM demonstrated superior or<br />
equivalent contrast of mass, and the same applied in most cases of microcalcifications. The margin of the<br />
mass was better defined in two cases, but both systems were the same when it came to determining the type of<br />
microcalcification. The authors concluded that FFDM might be helpful for detecting masses and determining<br />
their edges but offered no advantages when determining the type of calcification.<br />
. Reasons for disagreement in interpretation of FFDM and SFM<br />
Venta et al 15 studied the causes of disagreement in interpretation between FFDM (GE Senographe 2000D) and<br />
SFM in a diagnostic setting. They concluded that a significant disagreement that affected follow up management<br />
was present in only 4% of breasts. The greatest source of disagreement was found to be the radiologists’ management<br />
approach, which was more significant than differences in lesion visibility between the modalities.<br />
. Other techniques in digital mammography<br />
Digital mammography systems enable the development of new techniques for better breast cancer detection<br />
and diagnosis. Examples are contrast enhanced digital mammography, dual energy contrast enhanced digital<br />
subtraction mammography and tomosynthesis.<br />
3.4.1 Contrast enhanced digital mammography<br />
Contrast enhanced digital mammography utilises the principle that tumour growth and metastatic potential<br />
are directly linked to angiogenesis. 16 Contrast agents are administered and, as they distribute through the<br />
NHSBSP December 2005 9
Review of Literature on Digital Mammography in Screening<br />
blood, x-ray imaging shows increased contrast in the areas where they concentrate. Jong et al 16 have reported<br />
on early clinical experience with this method, suggesting that it may be useful in improving the conspicuity<br />
of lesions in dense tissue. In their study, 22 women who were scheduled for biopsy underwent contrast<br />
enhanced digital mammography. Six sequential images of the affected breast were obtained with a contrast<br />
agent injected intravenously between the time the first and the second image were obtained. Image processing<br />
included registration and logarithmic subtraction.<br />
A number of other studies have also investigated this new technique, concluding that contrast enhanced digital<br />
mammography has the potential of improving the visualisation of breast tumours and that it can be a useful<br />
tool in the detection and differentiation of benign and malignant lesions. 17–20<br />
3.4.2 Dual energy contrast enhanced digital subtraction mammography<br />
Dual energy contrast enhanced digital subtraction mammography is a method of breast angiography. This<br />
technique consists of high and low energy digital mammography after administration of iodinated contrast<br />
agent. Weighted subtraction of the logarithmic transform of the images is then performed and the final image<br />
preferentially shows iodine. 21,22 A study was performed of 26 patients with mammographic or clinical findings<br />
that warranted biopsy. 21 The results showed that 13 patients had invasive cancers, 11 of which enhanced<br />
strongly, one enhanced moderately and one weakly. One patient had ductal carcinoma in situ with the duct<br />
enhancing weakly. In the other 12 patients, benign tissue enhanced diffusely in two and weakly focally in two.<br />
These results indicate that this technique is useful and that further studies ought to be carried out. Another<br />
study compared contrast materials and reached the conclusion that zirconium (Zr) might be a better contrasting<br />
element than iodine for digital subtraction mammography. 22<br />
3.4.3 Tomosynthesis<br />
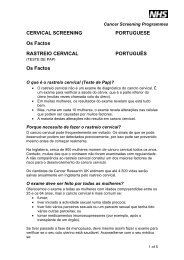
Tomosynthesis is a method of obtaining three dimensional images of a breast by acquiring a number of low<br />
radiation projection images while the x-ray source of a mammography system moves in an arc above the<br />
Figure Tomosynthesis acquisition geometry. 27<br />
NHSBSP December 2005 0
NHSBSP December 2005<br />
Review of Literature on Digital Mammography in Screening<br />
breast (Figure 1) either with the detector stationary or with the detector moving in the opposite direction to<br />
the x-ray tube. The individual images can then be reconstructed into a series of high resolution slices. 23 In this<br />
way, different planes of the breast can be displayed, which reduces tissue overlap, making the detectability<br />
of lesions easier. Any plane of the breast can be brought into focus, whereas structures outside this plane are<br />
blurred. 20 With this technique, important morphological information is not lost, making diagnosis easier and<br />
more accurate and, at the same time, reducing the number of recalls and biopsies. The total dose for tomosynthesis<br />
is claimed to be similar to or even lower than that required for standard screening mammography<br />
owing to the elimination of multiple exposures and reduced recalls. 24 Tomosynthesis can play an important<br />
role in screening because it offers the possibilities of reduced breast compression, improved diagnostic and<br />
screening accuracy, three dimensional lesion localisation and contrast enhanced three dimensional imaging. 23–25<br />
Comparisons between tomosynthesis methods and conventional two dimensional mammography have shown<br />
that tomosynthesis exhibits better contrast detail trends and higher detection scores. 25,26<br />
3.4.4 Breast computerised tomography<br />
One of the disadvantages of conventional mammography is that the superimposition of structures sometimes<br />
makes it difficult to detect small carcinomas. Although it is well known that computerised tomography (CT)<br />
is better in terms of contrast resolution than projection radiography by a factor of 10, traditional CT systems<br />
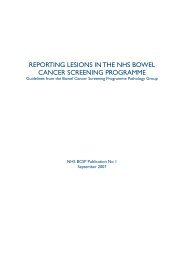
cannot be used for breast screening because of unnecessary irradiation of the thoracic cavity. 28 With cone beam<br />
breast CT (Figure 2), using flat panel detectors, three dimensional breast images could be obtained, resulting in<br />
better diagnostic images without the discomfort of breast compression and without unwanted exposure of the<br />
thoracic cavity. The breast is scanned in the pendulant position with the x-ray tube and detector arrays rotating<br />
around it. The detectors are placed just below the bottom of the shielded table and a swale is engineered<br />
around the area of the breast. In this way, breast tissue close to the thoracic wall and the axilla are imaged,<br />
avoiding unnecessary exposure. 28 A number of tests and simulations have shown that, with a mean glandular<br />
dose equivalent or lower than that of two view screening mammography, breast CT is capable of providing<br />
images with significantly better low contrast detectability of breast tumours and more accurate location of<br />
breast lesions. It has also been shown that objects that are 2 mm in diameter can be easily detected and that<br />
the optimal pixel size of the detector is around 0.2 mm. 28–32<br />
Figure 2 A CT scanner customised for breast imaging. 28
. C<strong>ON</strong>CLUSI<strong>ON</strong>S<br />
Review of Literature on Digital Mammography in Screening<br />
There is now strong evidence in the medical literature that FFDM achieves a diagnostic accuracy in screening<br />
that is at least as good as traditional SFM. Until recently, the published evidence was largely obtained using<br />
General Electric (GE) digital machines, as for the two Oslo trials. However, the recently published DMIST<br />
trial also demonstrated this result using a variety of manufacturers’ products. The DMIST trial is important<br />
because of the large number of women screened. This has allowed the equivalence of FFDM to SFM to be<br />
demonstrated with a much greater precision than in earlier trials. The DMIST trial also demonstrated for the<br />
first time that FFDM can be superior to SFM for important subgroups. The DMIST study reported finding<br />
no difference in clinical results between the different manufacturers’ systems. All of the systems used were<br />
carefully tested to ensure that they met the minimum criteria that apply in the USA.<br />
The authors of the Oslo trial used a methodology that is rather similar to the way in which screening is organised<br />
in the UK, so their results may be particularly pertinent to the UK context. The authors stress the importance<br />
of having good viewing conditions and of following a strict reading protocol. Both of these issues imply the<br />
need for careful training for radiologists switching from analogue to digital imaging. There seems to be no<br />
clear evidence that overall recall rates are likely to be any different from those found using the traditional<br />
equipment. The Oslo II trial reported relatively low recall rates for both SFM and FFDM and, consequently,<br />
high positive predictive values.<br />
NHSBSP December 2005 2
REFERENCES<br />
NHSBSP December 2005<br />
Review of Literature on Digital Mammography in Screening<br />
1. NHS Connecting for Health Picture Archiving and Communications (PACS) strategy. http://www.connectingforhealth.nhs.<br />
uk/publications/toolkitaugust05/factsheetpacs.doc and http://www.connectingforhealth.nhs.uk/pacs<br />
2. Lewin JM, Hendrick RE, D’Orsi CJ et al. Comparison of full-field digital mammography with screen-film mammography for<br />
cancer detection: results of 4,945 paired examinations. Radiology, 2001, 218, 873–880.<br />
3. Lewin JM, D’Orsi CJ, Hendrick RE et al. Clinical comparison of full-field digital mammography and screen-film<br />
mammography for detection of breast cancer. American Journal of Roentgenology, 2002, 179, 671–677.<br />
4. Skaane P, Young K. Population-based mammography screening: comparison of screen-film and full-field digital<br />
mammography with soft-copy reading: the Oslo I study. Radiology, 2003, 229, 877–884.<br />
5. Skaane P, Skjennald A. Screen-film mammography versus full-field digital mammography with soft-copy reading: randomized<br />
trial in a population-based screening program: the Oslo II study. Radiology, 2004, 232, 197–204.<br />
6. Pisano ED, Gatsonis CA, Yaffe MJ et al. The American College of Radiology Imaging Network Digital Mammographic<br />
Imaging Screening Trial: objectives and methodology. Radiology, 2005, 236, 404–412.<br />
7. Pisano ED, Gatsonis C, Hendrick E et al. Diagnostic performance of digital versus film mammography for breast-cancer<br />
screening. New England Journal of Medicine, 2005, 353, 1773–1783.<br />
8. Fischer U, Baum F, Obenauer S et al. Comparative study in patients with microcalcifications: full-field mammography vs.<br />
screen-film mammography. European Radiology, 2002, 12, 2679–2683.<br />
9. Di Nubila B, Cassano E, Origgi D et al. Analogic versus digital mammographic examination a radiological study of mammary<br />
microcalcifications on 52 surgical samples. Radiology Medicine (Torino), 2003, 106 (4), 297–304.<br />
10. Rong XJ, Shaw CC, Johnston DA et al. Microcalcification detectability for four mammography detectors: flat-panel, CCD, CR<br />
and screen-film. Medical Physics Journal, 2002, 29 (9), 2052–2061.<br />
11. Lai CJ, Shaw CC, Whitman CC et al. Visibility of simulated microcalcifications: a hardcopy-based comparison of three<br />
mammographic systems. Medical Physics Journal, 2005, 32, 182–194.<br />
12. Obenauer S, Luftner-Nagel S, von Heyden D et al. Screen-film vs. full-field digital mammography: image quality, detectability<br />
and characterization of lesions. European Radiology, 2002, 12, 1697–1702.<br />
13. Fischmann A, Siegmann KC, Wersebe A et al. Comparison of full-field digital mammography and film-screen mammography:<br />
image quality and lesion detection. British Journal of Radiology, 2005, 78, 312–315.<br />
14. Yamada T, Ishibashi T, Sato A et al. Comparison of screen-film and full-field digital mammography: image contrast and lesion<br />
characterization. Radiation Medicine, 2003, 21 (4), 166–173.<br />
15. Venta LA, Hendrick RE, Adler YT et al. Rate and causes of disagreement in interpretation of full-field digital mammography<br />
and film-screen mammography in a diagnostic setting. American Journal of Radiology, 2001, 176, 1241–1248.<br />
16. Jong RA, Yaffe MJ, Skarpathiotakis M et al. Contrast-enhanced digital mammography: initial clinical experience. Radiology,<br />
2003, 228, 842–850.<br />
17. Diekmann F, Diekmann S, Jeunehomme S et al. Digital mammography using iodine-based contrast material: initial clinical<br />
experience with dynamic contrast medium enhancement. Investigative Radiology, 2005, 40 (7), 397–404.<br />
18. Diekmann F, Diekmann S, Taupitz M et al. Use of iodine-based contrast media in digital full-field mammography: initial<br />
experience. Fortschritte Röntgenstrahlen, 2003, 175(3), 342–345.<br />
19. Skarpathiotakis M, Yaffe MJ, Bloomquist AK et al. Development of contrast digital mammography. Medical Physics Journal,<br />
2002, 29 (10), 2419–2426.<br />
20. Niklason LT, Kopans DB, Humberg LM et al. Digital breast imaging: tomosynthesis and digital subtraction mammography.<br />
Breast Disease, 1998, 10 (3–4), 151–164.<br />
21. Lewin JM, Isaacs PK, Vance V, Larke FJ. Dual-energy contrast-enhanced digital subtraction mammography: feasibility.<br />
Radiology, 2003, 229, 261–268.<br />
22. Lawaczeck R, Diekmann F, Diekmann S et al. New contrast media designed for x-ray energy subtraction imaging in digital<br />
mammography. Investigative Radiology, 2003, 38 (9), 602–608.<br />
23. Niklason LT, Christian BT, Niklason LE et al. Digital tomosynthesis in breast imaging. Radiology, 1997, 205 (2), 399–406.<br />
24. Wu T, Stewart A, Stanton M et al. Tomographic mammography using a limited number of low-dose cone-beam projection<br />
images. Medical Physics, 2003, 30 (3), 365–380.<br />
25. Suryanarayanan S, Karellas A, Vendantham S. Comparison of tomosynthesis methods used with digital mammography.<br />
Academic Radiology, 2000, 7, 1085–1097.<br />
26. Webber RL, Underhill RL, Freimanis RI. A controlled evaluation of tuned-aperture computed tomography applied to digital<br />
spot mammography. Journal of Digital Imaging, 2000, 13, 90–97.<br />
27. Smith A. Full field breast tomosynthesis. www.hologic.com/wh/pdf/W-LM-TOMO_Tomosynthesis.pdf
NHSBSP December 2005<br />
Review of Literature on Digital Mammography in Screening<br />
28. Boone JM, Nelson TR, Lindfors KK, Seibert JA. Dedicated breast CT: radiation dose and image quality evaluation. Radiology,<br />
2001, 221, 657–667.<br />
29. Gong X, Vedula AA, Glick SJ. Microcalcification detection using cone-beam CT mammography with a flat-panel imager.<br />
Physics in Medical Biology, 2004, 49, 2183–2195.<br />
30. Chen B, Ning R. Cone-beam volume CT breast: feasibility study. Medical Physics, 2002, 29 (5), 755–770.<br />
31. Boone JM, Shah N, Nelson TR. A comprehensive analysis of DgN(CT) coefficients for pendant-geometry cone-beam breast<br />
computed tomography. Medical Physics, 2004, 31 (2), 226–235.<br />
32. Thacker SC, Glick SJ. Normalized glandular dose (DgN) coefficients for flat-panel CT breast imaging. Physics in Medical<br />
Biology, 2004, 49, 5433–5444.
BIBLIOGRAPHY<br />
Review of Literature on Digital Mammography in Screening<br />
Karssemaijer N, Thijssen M, Hendriks J, van Erning L (eds). Digital Mammography IWDM 1998, Proceedings of the 4th<br />
International Workshop on Digital Mammography. Dordrecht, Kluwer Academic Publishers, 1998.<br />
Peitgen HO (ed.). Digital Mammography IWDM 2002, Proceedings of the 6th International Workshop on Digital Mammography.<br />
Madison, WI, Medical Physics Publishing, 2003.<br />
Yaffe MJ (ed.). Digital Mammography IWDM 2000, Proceedings of the 5th International Workshop on Digital Mammography.<br />
Berlin, Springer-Verlag, 2001.<br />
NHSBSP December 2005 5
Review of Literature on Digital Mammography in Screening<br />
NHSBSP December 2005 6