

Book of Medical Disorders in Pregnancy - Tintash
Book of Medical Disorders in Pregnancy - Tintash
Book of Medical Disorders in Pregnancy - Tintash

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
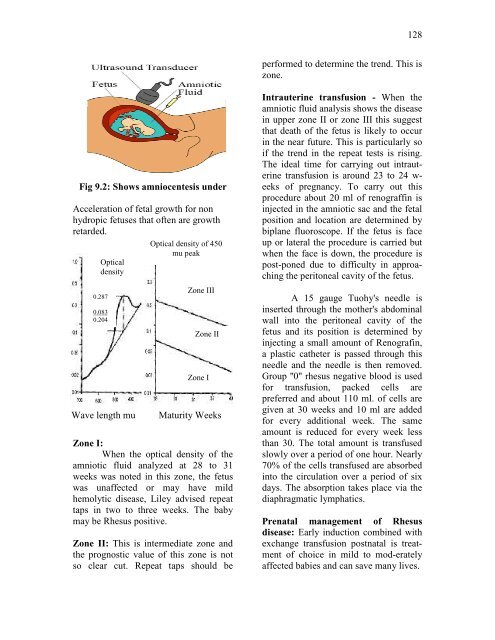
Fig 9.2: Shows amniocentesis under<br />
Acceleration <strong>of</strong> fetal growth for non<br />
hydropic fetuses that <strong>of</strong>ten are growth<br />
retarded.<br />
Optical<br />
density<br />
0.287<br />
0.083<br />
0.204<br />
Wave length mu<br />
Optical density <strong>of</strong> 450<br />
mu peak<br />
Zone III<br />
Zone II<br />
Zone I<br />
Maturity Weeks<br />
Zone I:<br />
When the optical density <strong>of</strong> the<br />
amniotic fluid analyzed at 28 to 31<br />
weeks was noted <strong>in</strong> this zone, the fetus<br />
was unaffected or may have mild<br />
hemolytic disease, Liley advised repeat<br />
taps <strong>in</strong> two to three weeks. The baby<br />
may be Rhesus positive.<br />
Zone II: This is <strong>in</strong>termediate zone and<br />
the prognostic value <strong>of</strong> this zone is not<br />
so clear cut. Repeat taps should be<br />
128<br />
performed to determ<strong>in</strong>e the trend. This is<br />
zone.<br />
Intrauter<strong>in</strong>e transfusion - When the<br />
amniotic fluid analysis shows the disease<br />
<strong>in</strong> upper zone II or zone III this suggest<br />
that death <strong>of</strong> the fetus is likely to occur<br />
<strong>in</strong> the near future. This is particularly so<br />
if the trend <strong>in</strong> the repeat tests is ris<strong>in</strong>g.<br />
The ideal time for carry<strong>in</strong>g out <strong>in</strong>trauter<strong>in</strong>e<br />
transfusion is around 23 to 24 weeks<br />
<strong>of</strong> pregnancy. To carry out this<br />
procedure about 20 ml <strong>of</strong> renograff<strong>in</strong> is<br />
<strong>in</strong>jected <strong>in</strong> the amniotic sac and the fetal<br />
position and location are determ<strong>in</strong>ed by<br />
biplane fluoroscope. If the fetus is face<br />
up or lateral the procedure is carried but<br />
when the face is down, the procedure is<br />
post-poned due to difficulty <strong>in</strong> approach<strong>in</strong>g<br />
the peritoneal cavity <strong>of</strong> the fetus.<br />
A 15 gauge Tuohy's needle is<br />
<strong>in</strong>serted through the mother's abdom<strong>in</strong>al<br />
wall <strong>in</strong>to the peritoneal cavity <strong>of</strong> the<br />
fetus and its position is determ<strong>in</strong>ed by<br />
<strong>in</strong>ject<strong>in</strong>g a small amount <strong>of</strong> Renograf<strong>in</strong>,<br />
a plastic catheter is passed through this<br />
needle and the needle is then removed.<br />
Group ''0'' rhesus negative blood is used<br />
for transfusion, packed cells are<br />
preferred and about 110 ml. <strong>of</strong> cells are<br />
given at 30 weeks and 10 ml are added<br />
for every additional week. The same<br />
amount is reduced for every week less<br />
than 30. The total amount is transfused<br />
slowly over a period <strong>of</strong> one hour. Nearly<br />
70% <strong>of</strong> the cells transfused are absorbed<br />
<strong>in</strong>to the circulation over a period <strong>of</strong> six<br />
days. The absorption takes place via the<br />
diaphragmatic lymphatics.<br />
Prenatal management <strong>of</strong> Rhesus<br />
disease: Early <strong>in</strong>duction comb<strong>in</strong>ed with<br />
exchange transfusion postnatal is treatment<br />
<strong>of</strong> choice <strong>in</strong> mild to mod-erately<br />
affected babies and can save many lives.