Noise-Induced Hearing Loss - American Academy of Audiology
Noise-Induced Hearing Loss - American Academy of Audiology
Noise-Induced Hearing Loss - American Academy of Audiology

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Assessing <strong>Hearing</strong> Protectors in the<br />
Clinic- How to Perform CPT 92596<br />
Assessing <strong>Hearing</strong> Protectors<br />
in the Clinic:<br />
How to Perform CPT Code 92596<br />
Tom Thunder, AuD, FAAA, INCE Bd. Cert.<br />
Audiologist and Acoustical Specialist<br />
Northern Illinois University, DeKalb, IL<br />
Acoustic Associates, Palatine, Illinois<br />
Interacts with …<br />
• Smoking<br />
• Paint solvents (toluene)<br />
• Carbon monoxide (CO)<br />
• Strenuous exercise<br />
State <strong>of</strong> Washington<br />
Workers’ Compensation<br />
Claims for <strong>Hearing</strong> <strong>Loss</strong><br />
• Increased nearly 12-fold during 1984-1998.<br />
• 90% <strong>of</strong> the claimants received permanent<br />
partial disability compensation.<br />
• Identifiable costs exceeded $57 million<br />
dollars in 1998.<br />
“…occupational hearing loss is probably much more<br />
common than usually recognized, and contemporary workers<br />
may still face substantial risk for hearing loss.”<br />
Based on 27,019 claims filed<br />
Acoustic Associates, Ltd.<br />
Tom Thunder, AuD, INCE ( tthunder@comcast.net)<br />
Daniell et al. Am J Ind Med.<br />
2002 Dec;42(6):502-10.<br />
Excess Risk in %<br />
<strong>American</strong> <strong>Academy</strong> <strong>of</strong><br />
<strong>Audiology</strong> (April 2009)<br />
<strong>Noise</strong>-<strong>Induced</strong> <strong>Hearing</strong> <strong>Loss</strong><br />
50<br />
40<br />
30<br />
20<br />
10<br />
0<br />
1<br />
8<br />
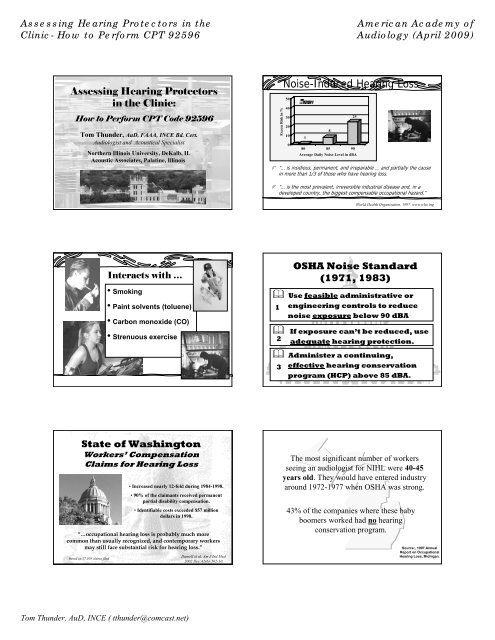
“… is insidious, permanent, and irreparable … and partially the cause<br />
in more than 1/3 <strong>of</strong> those who have hearing loss.<br />
“… is the most prevalent, irreversible industrial disease and, in a<br />
developed country, the biggest compensable occupational hazard.”<br />
25<br />
80 85 90<br />
Average Daily <strong>Noise</strong> Level in dBA<br />
World Health Organization, 1997. www.who.ing<br />
OSHA <strong>Noise</strong> Standard<br />
(1971, 1983)<br />
Use feasible administrative or<br />
1 engineering controls to reduce<br />
noise exposure below 90 dBA<br />
If exposure can’t be reduced, use<br />
2 adequate hearing protection.<br />
Administer a continuing,<br />
3<br />
effective hearing conservation<br />
program (HCP) above 85 dBA.<br />
The most significant number <strong>of</strong> workers<br />
seeing an audiologist for NIHL were 40-45<br />
years old. They would have entered industry<br />
around 1972-1977 when OSHA was strong.<br />
43% <strong>of</strong> the companies where these baby<br />
boomers worked had no hearing<br />
conservation program.<br />
Source:, 1997 Annual<br />
Report on Occupational<br />
<strong>Hearing</strong> <strong>Loss</strong>, Michigan.
Assessing <strong>Hearing</strong> Protectors in the<br />
Clinic- How to Perform CPT 92596<br />
Bureau <strong>of</strong> Labor and Statistics<br />
Occupational Injuries for 2007<br />
<strong>Hearing</strong> loss was the 2 nd highest specific reported<br />
illness in all <strong>of</strong> the last four years since OSHA has<br />
required separate reporting <strong>of</strong> hearing loss.<br />
<strong>Hearing</strong> Protection Devices<br />
workplace noise effective employee exposure<br />
A-Weighted Sound Level (dBA)<br />
125<br />
115<br />
105<br />
95<br />
85<br />
dBC - NRR = dBA<br />
C – A Differences<br />
Mean C-A = 2 dB<br />
-2 0 2 4 6 8 10 12 14<br />
C - A Value (dB)<br />
Combined Industrial <strong>Noise</strong>s<br />
Special <strong>Noise</strong>s (see text)<br />
C-A > 7 dB = 4%<br />
Linear Curve<br />
Tom Thunder, AuD, INCE ( tthunder@comcast.net)<br />
Relative Sound Pressure Level in dB<br />
Over Reliance on <strong>Hearing</strong><br />
Protection Devices<br />
With OSHA’s lax<br />
enforcement policy<br />
<strong>of</strong> the 80s,<br />
management <strong>of</strong> the<br />
90s and beyond<br />
have relied on<br />
protection to the<br />
extent that if HPDs<br />
were issued, the<br />
noise problem<br />
vanished.<br />
20<br />
10<br />
0<br />
-10<br />
-20<br />
-30<br />
-40<br />
-50<br />
-60<br />
-70<br />
-80<br />
16<br />
Weighting Scales<br />
31.5<br />
63<br />
125<br />
250<br />
<strong>American</strong> <strong>Academy</strong> <strong>of</strong><br />
<strong>Audiology</strong> (April 2009)<br />
500<br />
1000<br />
Frequency in Hz<br />
2000<br />
4000<br />
8000<br />
C-weighting<br />
A-weighting<br />
Questionable Perception <strong>of</strong><br />
HPD Performance<br />
Most HR<br />
<strong>of</strong>ficers and<br />
safety<br />
managers<br />
believe that<br />
the higher the<br />
NRR, better<br />
the<br />
protection.<br />
NRR (dB)<br />
30<br />
25<br />
20<br />
15<br />
10<br />
5<br />
0<br />
Labeled vs. Field Values<br />
Down<br />
Custom<br />
Laboratory<br />
Field<br />
16000<br />
Sound-Ban 10/20<br />
UltraFit<br />
V-51R<br />
POP/S<strong>of</strong>t<br />
EP-100<br />
Misc. 3-flange<br />
Classic<br />
Peltor H9A<br />
Misc. M uffs<br />
M SA Mk IV<br />
Hlbrg. No-<strong>Noise</strong><br />
Bilsom 2313<br />
Peltor H7P3e<br />
Bilsom UF-1
Assessing <strong>Hearing</strong> Protectors in the<br />
Clinic- How to Perform CPT 92596<br />
NRR (dB)<br />
Real-Ear Attenuation (dB)<br />
Using the NRR<br />
Not Really Right<br />
dBA P =dBA w – ½ (NRR – 7)<br />
workplace noise<br />
protected employee exposure<br />
• 50% derating: a safety margin to account for the field vs.<br />
lab difference in the labeled NRR.<br />
• 7-dB correction: another safety margin to account for the<br />
spectral uncertainty (i.e., the difference between the C<br />
and A weighted levels).<br />
35<br />
30<br />
25<br />
20<br />
15<br />
10<br />
5<br />
0<br />
-10<br />
0<br />
10<br />
20<br />
30<br />
40<br />
Predicted vs. Field Values<br />
V-51R<br />
EP-100<br />
Field<br />
S<strong>of</strong>t<br />
Custom<br />
Method B<br />
SoundBan<br />
Com-Fit<br />
UltraFit<br />
Mark IV<br />
H7P3E<br />
Classic<br />
H9A<br />
UF-1<br />
Classic+UF-1<br />
Attenuation Data<br />
Tom Thunder, AuD, INCE ( tthunder@comcast.net)<br />
Label Test<br />
50<br />
.125 .250 .500 1.0 2.0 4.0 8.0<br />
Frequency (kHz)<br />
0<br />
15 Std. Dev.<br />
ANSI S12.6 -1997 (R2002)<br />
REAT<br />
(Real-Ear at Threshold)<br />
ANSI S12.6 – 1997<br />
(R2002)<br />
Sound-field thresholds<br />
measured without HPD<br />
Sound-field thresholds<br />
measured with HPD<br />
The difference is the<br />
attenuation <strong>of</strong> the HPD<br />
(insertion loss)<br />
<strong>American</strong> <strong>Academy</strong> <strong>of</strong><br />
<strong>Audiology</strong> (April 2009)<br />
Method A:<br />
- Fit by tester<br />
- 10 experienced subjects<br />
- 3 trials (30 runs)<br />
Method B:<br />
- Fit by subject<br />
- 20 naïve subjects<br />
- 2 trials (40 runs)<br />
Laboratory Testing <strong>of</strong> HPDs<br />
Reverberant Room<br />
1/3<br />
1/3-Octaveband <strong>Noise</strong> Signal<br />
Best Practice Bulletin:<br />
<strong>Hearing</strong> Protection-Emerging Trends: Individual Fit Testing<br />
Any population-based statistical estimate <strong>of</strong> hearing<br />
protector performance is a poor estimate <strong>of</strong> individual<br />
performance.<br />
If the purpose <strong>of</strong> HPD evaluation is to determine how well<br />
specific HPDs work on specific people, then they must be<br />
tested on individual people (similar to the quantitative fit<br />
testing <strong>of</strong> respirators).<br />
http://www.hearingconservation.org/docs/AllianceRecommendationForFitTesting_Final.pdf
Assessing <strong>Hearing</strong> Protectors in the<br />
Clinic- How to Perform CPT 92596<br />
Ear Protector Attenuation Measurement<br />
An assessment <strong>of</strong> ear protector performance for a specific ear<br />
protector on a specific individual. Why do it?<br />
Fit verification – to verify “adequacy” <strong>of</strong> fit<br />
STS evaluations – to assess poor fit as a potential<br />
contribution to the change in hearing<br />
Work-related evaluation – to factor in HPD use<br />
Training and education – an OSHA required<br />
component <strong>of</strong> an effective HCP<br />
HPD selection – and aid in selecting a good HPD for new<br />
employees<br />
Documentation – establishes evidence that HPDs were<br />
selected and fit for legal records<br />
EARfit ® Technology<br />
Dual element<br />
microphone<br />
Simultaneous<br />
measurement inside<br />
and outside HPD yields<br />
noise reduction (NR)<br />
Specially prepared<br />
protector called a<br />
“probed HPD”<br />
Advantages<br />
F-Mire Approach<br />
Quick – 8 seconds per ear<br />
Objective (non-linear HPDs)<br />
Can test one or both ears<br />
Quiet is not needed<br />
<strong>Hearing</strong> loss not an issue<br />
Great documentation<br />
Tests at 125 and 8000 Hz<br />
Disadvantages<br />
Tom Thunder, AuD, INCE ( tthunder@comcast.net)<br />
Cost<br />
Space<br />
Can only test<br />
manufacturer’s HPDs<br />
Special probed HPDs<br />
Acoustic flanking at high<br />
frequencies<br />
For a short movie clip, see: http://www.e-a-rfit.com/process.aspx<br />
<strong>American</strong> <strong>Academy</strong> <strong>of</strong><br />
<strong>Audiology</strong> (April 2009)<br />
F-MIRE (Field Microphone in Real-Ear)<br />
Utilizes the same real-ear approach to<br />
verifying the insertion gain <strong>of</strong> hearing<br />
aids, except here you are measuring the<br />
insertion loss <strong>of</strong> earplugs.<br />
Individual HPD Fit Test:<br />
EARfit ® Technology<br />
S<strong>of</strong>tware provides the stimulus, calculations, and<br />
ear-canal-to-sound-field transfer function.<br />
Loudness Balance<br />
The VeriPRO uses a 3-part<br />
loudness balance process to<br />
measure the attenuation <strong>of</strong> a<br />
patient’s earplug fit in each ear<br />
over a range <strong>of</strong> 5 frequencies.<br />
With this real-world data, you<br />
can find out whether your<br />
patient is receiving optimal<br />
protection, requires additional<br />
training on how to fit their<br />
earplugs, or if they need to try a<br />
different model.
Assessing <strong>Hearing</strong> Protectors in the<br />
Clinic- How to Perform CPT 92596<br />
Developed in conjunction<br />
with the House Ear<br />
Institute and uses<br />
sophisticated s<strong>of</strong>tware in a<br />
user-friendly format to<br />
determine the Personal<br />
Attenuation Rating (PAR)<br />
your patient receives.<br />
The VeriPRO package<br />
consists <strong>of</strong> PC-based<br />
s<strong>of</strong>tware, an audio<br />
processor, a USB cable,<br />
and an audiometrically<br />
optimized headset.<br />
Renee Besette <strong>of</strong> Howard Leight<br />
by Sperian takes a visitor<br />
through this simple audio<br />
demonstration<br />
http://www.ohscanada.com/ohstv/Howard-Leight-NSC-2007.asp<br />
Five frequencies are balanced (250, 500, 1k, 2k and 4k Hz)<br />
Using the mouse, raise or lower<br />
the slider bar until the volume<br />
in your left ear matches the<br />
volume in your right ear (which<br />
always stays the same).<br />
Compare the volume only, not<br />
the quality or pitch <strong>of</strong> the tone.<br />
When you have reached a<br />
balance, click MATCH to move<br />
on to the next frequency.<br />
First, a balance is done to get an unprotected reference level for the left ear.<br />
Second, a plug is inserted in the right ear and a balance is done to determine the<br />
PAR for the right plug.<br />
Third, a plug is inserted in the left ear and a balance is done to determine the PAR<br />
for the left plug (measures the change in level on the left).<br />
A color visual is given to show how well a specific<br />
protector works for that patient.<br />
Tom Thunder, AuD, INCE ( tthunder@comcast.net)<br />
<strong>American</strong> <strong>Academy</strong> <strong>of</strong><br />
<strong>Audiology</strong> (April 2009)<br />
In this approach, users match the volume <strong>of</strong> a tone in one ear to the other ear.<br />
Informational graphics and instructional text guide the user through the process.<br />
At the end <strong>of</strong> a Check, users view a report giving the patient’s PAR<br />
for the HPD worn. The report can be printed or saved as a PDF.<br />
Loudness Balance Approach<br />
Advantages<br />
Pr<strong>of</strong>essional efficiency<br />
Works with any earplug<br />
Tests both ears<br />
Good documentation<br />
Quiet not needed<br />
Disadvantages<br />
Cost - $2,900<br />
Space<br />
Won’t work with muffs or caps<br />
Subjective<br />
<strong>Hearing</strong> loss can be an issue<br />
Relatively slow – 9 min
Assessing <strong>Hearing</strong> Protectors in the<br />
Clinic- How to Perform CPT 92596<br />
REAT (Real-Ear at Threshold)<br />
Based on ANSI S12.6 (a lab standard).<br />
Audiometric<br />
Room<br />
Warbled Pure Tone Signal<br />
Advantages<br />
Tom Thunder, AuD, INCE ( tthunder@comcast.net)<br />
Sound-Field<br />
thresholds are<br />
measured without the<br />
HPD<br />
Sound-Field<br />
thresholds are then<br />
measured with HPD<br />
The difference is the<br />
attenuation <strong>of</strong> the<br />
HPD (insertion loss)<br />
PAR Patient ©- a Micros<strong>of</strong>t Excel ® Template<br />
<strong>American</strong> <strong>Academy</strong> <strong>of</strong><br />
<strong>Audiology</strong> (April 2009)<br />
Why don’t audiologists measure HPD performance?<br />
Most audiologists have the capability to measure attenuation …<br />
they just don’t know how to calculate the individual NRR (called<br />
the Personal Attenuation Rating).<br />
Originally developed to give students a lab exercise.<br />
Automatically calculates the patient’s PAR<br />
Active Link to Look up the HPD’s laboratory NRR (NIOSH)<br />
Active Link to Look up noise levels (AEARO database)<br />
Estimates the effective (protected) noise level<br />
Generates a range <strong>of</strong> protected noise levels based on the<br />
probable frequency spectrum <strong>of</strong> the patient’ s exposure<br />
Available from: Acoustic Associates (info@AcousticAssociates.com)<br />
Printed Document (Upper Half) Printed Document (Lower Half)<br />
REAT Approach<br />
A common clinical test<br />
Follows the REAT method<br />
<strong>of</strong> the ANSI standard<br />
Negligible cost<br />
Works with any HPD<br />
Disadvantages<br />
Relatively slow – 8 min<br />
Subjective<br />
Binaural measure<br />
<strong>Hearing</strong> loss can be an<br />
issue<br />
No one needs to lose<br />
his or her hearing in<br />
order to earn a living.<br />
<strong>Noise</strong>-induced hearing<br />
loss is preventable.<br />
<strong>Noise</strong>-induced hearing loss<br />
remains one <strong>of</strong> the most<br />
prevalent occupational<br />
conditions and is found in a<br />
wide range <strong>of</strong> industries.