144 SEBORRHEIC DERMATITIS SECTION 8 PAPULOSQUAMOUS ...
144 SEBORRHEIC DERMATITIS SECTION 8 PAPULOSQUAMOUS ...
144 SEBORRHEIC DERMATITIS SECTION 8 PAPULOSQUAMOUS ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
MHBD125-<strong>144</strong>[615-619].qxd 8/18/08 5:48 PM Page 615<br />
<strong>144</strong> <strong>SEBORRHEIC</strong><br />
<strong>DERMATITIS</strong><br />
Richard P. Usatine, MD<br />
PATIENT STORY<br />
<strong>SEBORRHEIC</strong> <strong>DERMATITIS</strong><br />
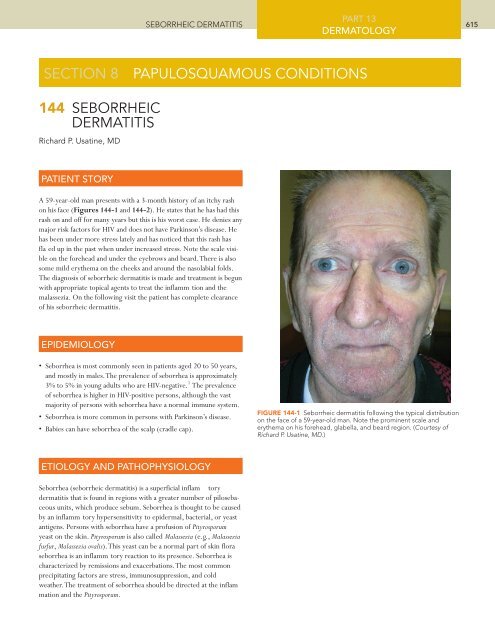
A 59-year-old man presents with a 3-month history of an itchy rash<br />
on his face (Figures <strong>144</strong>-1 and <strong>144</strong>-2). He states that he has had this<br />
rash on and off for many years but this is his worst case. He denies any<br />
major risk factors for HIV and does not have Parkinson’s disease. He<br />
has been under more stress lately and has noticed that this rash has<br />
fla ed up in the past when under increased stress. Note the scale visible<br />
on the forehead and under the eyebrows and beard.There is also<br />
some mild erythema on the cheeks and around the nasolabial folds.<br />
The diagnosis of seborrheic dermatitis is made and treatment is begun<br />
with appropriate topical agents to treat the inflamm tion and the<br />
malassezia. On the following visit the patient has complete clearance<br />
of his seborrheic dermatitis.<br />
EPIDEMIOLOGY<br />
• Seborrhea is most commonly seen in patients aged 20 to 50 years,<br />
and mostly in males.The prevalence of seborrhea is approximately<br />
3% to 5% in young adults who are HIV-negative. 1 The prevalence<br />
of seborrhea is higher in HIV-positive persons, although the vast<br />
majority of persons with seborrhea have a normal immune system.<br />
• Seborrhea is more common in persons with Parkinson’s disease.<br />
• Babies can have seborrhea of the scalp (cradle cap).<br />
ETIOLOGY AND PATHOPHYSIOLOGY<br />
Seborrhea (seborrheic dermatitis) is a superficial inflam tory<br />
dermatitis that is found in regions with a greater number of pilosebaceous<br />
units, which produce sebum. Seborrhea is thought to be caused<br />
by an inflamm tory hypersensitivity to epidermal, bacterial, or yeast<br />
antigens. Persons with seborrhea have a profusion of Pityrosporum<br />
yeast on the skin. Pityrosporum is also called Malassezia (e.g., Malassezia<br />
furfur, Malassezia ovalis).This yeast can be a normal part of skin flora<br />
seborrhea is an inflamm tory reaction to its presence. Seborrhea is<br />
characterized by remissions and exacerbations.The most common<br />
precipitating factors are stress, immunosuppression, and cold<br />
weather.The treatment of seborrhea should be directed at the inflam<br />
mation and the Pityrosporum.<br />
PART 13<br />
DERMATOLOGY<br />
<strong>SECTION</strong> 8 <strong>PAPULOSQUAMOUS</strong> CONDITIONS<br />
FIGURE <strong>144</strong>-1 Seborrheic dermatitis following the typical distribution<br />
on the face of a 59-year-old man. Note the prominent scale and<br />
erythema on his forehead, glabella, and beard region. (Courtesy of<br />
Richard P. Usatine, MD.)<br />
615
MHBD125-<strong>144</strong>[615-619].qxd 8/18/08 5:48 PM Page 616<br />
PART 13<br />
616 CHAPTER <strong>144</strong><br />
DERMATOLOGY<br />
DIAGNOSIS<br />
The diagnosis is made on history and physical examination. Figures<br />
<strong>144</strong>-1 and <strong>144</strong>-2 reveal erythema and scale across the eyebrows,<br />
cheeks, and under beard.<br />
CLINICAL FEATURES<br />
• Seborrhea on the face and scalp can be very pruritic.<br />
• Plaques of greasy scale are visible in the seborrheic distribution.<br />
• In dark-skinned individuals, the involved skin and scale may become<br />
hyperpigmented (Figure <strong>144</strong>-3).<br />
• The more severe the seborrhea, the thicker and greasier the scale<br />
(Figure <strong>144</strong>-4).<br />
• Infants may develop seborrhea on the scalp, known as cradle cap<br />
(Figure <strong>144</strong>-5).They may also have seborrhea on the face around<br />
the eyebrows (Figure <strong>144</strong>-6). Some infants have a wider distribution<br />
involving the neck creases, armpits, or groin.<br />
TYPICAL DISTRIBUTION<br />
Scalp (i.e., dandruff), eyebrows (Figures <strong>144</strong>-6 and <strong>144</strong>-7),<br />
nasolabial creases, forehead, cheeks, around the nose, behind the ears<br />
(Figure <strong>144</strong>-8), and under facial hair (Figure <strong>144</strong>-9). Seborrhea can<br />
also occur over the sternum and in the axillae, submammary folds,<br />
umbilicus, groin, and gluteal creases.<br />
LABORATORY STUDIES<br />
HIV test if history is suspicious.<br />
DIFFERENTIAL DIAGNOSIS<br />
• SLE with butterf y rash—rash across bridge of nose in patient with<br />
other systemic abnormalities and abnormal blood tests (Chapter<br />
173, Lupus Erythematosus - Systemic and Cutaneous).<br />
• Rosacea—the erythema on the face is often associated with<br />
papules, pustules and possibly chalazia or hordeola (Chapter 107,<br />
Rosacea).<br />
• Psoriasis —the scale of psoriasis tends to be thicker and distributed<br />
over extensor surfaces along with the scalp. Look for signs of nail<br />
involvement that support the diagnosis of psoriasis. (Chapter 145,<br />
Psoriasis).<br />
• Tinea capitis—usually has hair loss with the scale and erythema.<br />
KOH and/or culture can help make the distinction (Chapter 131,<br />
Tinea Capitis).<br />
MANAGEMENT<br />
• Treat the Malassezia with antifungals:<br />
~ Shampoos containing ketoconazole, selenium sulfide or zin<br />
pyrithione (ZPT) are active against the Malassezia and are effective<br />
in the treatment of moderate to severe dandruff. 2,3 SOR <br />
~ Ketoconazole 2% shampoo was found to be superior to zinc<br />
pyrithione 1% shampoo when used twice weekly. Ketoconazole<br />
FIGURE <strong>144</strong>-2 Close-up of seborrheic dermatitis showing the flaking<br />
scale and erythema around the beard region. (Courtesy of Richard P.<br />
Usatine, MD.)<br />
FIGURE <strong>144</strong>-3 Seborrhea in a black woman with hyperpigmentation<br />
related to the inflammation. Note the prominent involvement in the<br />
nasolabial folds. (Courtesy of Richard P. Usatine, MD.)
MHBD125-<strong>144</strong>[615-619].qxd 8/18/08 5:49 PM Page 617<br />
led to a 73% improvement in the total dandruff severity score<br />
compared with 67% for ZPT 1% at 4 weeks. 3 SOR <br />
~ Ciclopirox shampoo 1% is effective and safe in the treatment of<br />
seborrheic dermatitis of the scalp. 4,5 SOR It is by prescription<br />
only and is very expensive.<br />
~ 2% ketoconazole cream, gel, or emulsion is safe and effective for<br />
facial seborrheic dermatitis. 6–8 SOR <br />
~ 1% ciclopirox cream is also safe and effective for facial seborrheic<br />
dermatitis and is equivalent to 2% ketoconazole cream. 6,9<br />
SOR <br />
~ Oral terbinafine 250 mg dai y for 4 weeks is effective for moderate<br />
to severe seborrhea. 10,11 SOR <br />
• Treat the inflamm tion using topical steroids<br />
~ Lotion or solution is preferable on hair-covered area for patient<br />
comfort and usability.<br />
~ 1% Hydrocortisone cream or lotion can be used bid to face,<br />
scalp, or other affected areas. 8,12 SOR <br />
~ Desonide 0.05% lotion is safe and effective for short-term treatment<br />
of seborrheic dermatitis of the face. 13 SOR It is a nonflu<br />
orinated low to mid-potency steroid that is higher in potency<br />
than 1% hydrocortisone.<br />
~ For moderate to severe seborrhea on the scalp.<br />
■ 0.05% Fluocinonide solution once daily is affordable and beneficial<br />
SOR <br />
■ 0.05% Clobetasol shampoo, solution, spray, or foam work well<br />
but are more costly. SOR <br />
OTHER TREATMENTS<br />
• Pimecrolimus cream 1% is an effective and well-tolerated<br />
treatment for facial seborrheic dermatitis. 12,14,15 SOR In one<br />
study, there was more burning noted with the pimecrolimus than<br />
the betamethasone 17-valerate 0.1% cream. 14<br />
• Metronidazole Gel—two small studies have found different results<br />
in the treatment of seborrheic dermatitis on the face. One suggests<br />
it works better than the vehicle alone and the other found no statistically<br />
significant diffe ence from the placebo. 16,17 SOR <br />
• Tea tree oil 5% shampoo showed a 41% improvement in the quadrant-area-severity<br />
score compared with 11% in the placebo. Statistically<br />
significant imp ovements were also observed in the total area<br />
of involvement score, the total severity score, and the itchiness and<br />
greasiness components of the patients’ self-assessments. 18 SOR <br />
• One small RCT (with high drop-out rate) using homeopathic medication<br />
consisting of potassium bromide, sodium bromide, nickel<br />
sulfate, and sodium chloride for 10 weeks showed significan<br />
improvement over placebo. 19 SOR <br />
PATIENT EDUCATION<br />
<strong>SEBORRHEIC</strong> <strong>DERMATITIS</strong><br />
For improved treatment results, encourage patients to wash the hair<br />
and scalp daily with an antifungal shampoo. Some patients fear that<br />
washing their hair too often will cause a “dry” scalp and need to<br />
understand that the scaling and flaking will imp ove rather than<br />
worsen with more frequent hair washing.<br />
PART 13<br />
DERMATOLOGY<br />
FIGURE <strong>144</strong>-4 Severe seborrheic dermatitis on the face of a hospitalized<br />
man. The stress of his illness has worsened his otherwise mild seborrhea.<br />
(Courtesy of Richard P. Usatine, MD.)<br />
FIGURE <strong>144</strong>-5 Cradle cap in an infant that also has atopic dermatitis.<br />
(Courtesy of Richard P. Usatine, MD.)<br />
FIGURE <strong>144</strong>-6 Mild seborrheic dermatitis with subtle flaking around<br />
the eyebrows of a 2-month-old girl who also has cradle cap. (Courtesy<br />
of Richard P. Usatine, MD.)<br />
617
MHBD125-<strong>144</strong>[615-619].qxd 8/18/08 5:49 PM Page 618<br />
PART 13<br />
618 CHAPTER <strong>144</strong><br />
DERMATOLOGY<br />
FOLLOW-UP<br />
Patients with long-standing and severe seborrhea will appreciate a<br />
follow-up visit in most cases. Milder cases can be followed as needed.<br />
PATIENT RESOURCES<br />
VisualDxHealth - good information and photographs:<br />
http://www.visualdxhealth.com/adult/<br />
seborrheicDermatitis.htm.<br />
http://www.visualdxhealth.com/adult/dandruff.htm.<br />
PROVIDER RESOURCES<br />
eMedicine<br />
http://www.emedicine.com/derm/topic396.htm.<br />
DermNet NZ<br />
http://dermnetnz.org/dermatitis/seborrhoeicdermatitis.htm.<br />
REFERENCE<br />
1. Usatine RP.A red rash on the face. J Fam Pract. 2003;52:697–699.<br />
2. Danby FW, Maddin WS, Margesson LJ, Rosenthal D.A randomized,<br />
double-blind, placebo-controlled trial of ketoconazole 2%<br />
shampoo versus selenium sulfide 2.5% shampoo in the t eatment<br />
of moderate to severe dandruff. J Am Acad Dermatol. 1993;29:<br />
1008–1012.<br />
3. Pierard-Franchimont C.A multicenter randomized trial of ketoconazole<br />
2% and zinc pyrithione 1% shampoos in severe dandruff<br />
and seborrheic dermatitis. Skin Pharmacol Appl Skin Physiol. 2002;<br />
15(6):434–441.<br />
4. Aly R. Ciclopirox gel for seborrheic dermatitis of the scalp. Int J<br />
Dermatol.2003;42(Suppl 1):19–22.<br />
5. Lebwohl M, Plott T. Safety and effica y of ciclopirox 1% shampoo<br />
for the treatment of seborrheic dermatitis of the scalp in the US<br />
population: Results of a double-blind, vehicle-controlled trial. Int<br />
J Dermatol. 2004;43(Suppl 1):17–20.<br />
6. Chosidow O, Maurette C, Dupuy P. Randomized, open-labeled,<br />
non-inferiority study between ciclopiroxolamine 1% cream and<br />
ketoconazole 2% foaming gel in mild to moderate facial seborrheic<br />
dermatitis. Dermatology. 2003;206:233–240.<br />
7. Pierard GE, Pierard-Franchimont C,Van CJ, Rurangirwa A,<br />
Hoppenbrouwers ML, Schrooten P. Ketoconazole 2% emulsion<br />
in the treatment of seborrheic dermatitis. Int J Dermatol. 1991;30:<br />
806–809.<br />
8. Katsambas A,Antoniou C, Frangouli E,Avgerinou G, Michailidis<br />
D, Stratigos J.A double-blind trial of treatment of seborrhoeic<br />
dermatitis with 2% ketoconazole cream compared with 1%<br />
hydrocortisone cream. Br J Dermatol. 1989;121:353–357.<br />
9. Dupuy P, Maurette C,Amoric JC, Chosidow O. Randomized,<br />
placebo-controlled, double-blind study on clinical effica y of<br />
ciclopiroxolamine 1% cream in facial seborrhoeic dermatitis.<br />
Br J Dermatol. 2001;<strong>144</strong>:1033–1037.<br />
FIGURE <strong>144</strong>-7 Seborrheic dermatitis with erythema and scale under<br />
the eyebrows and in the glabella region on a young man. (Courtesy of<br />
Richard P. Usatine, MD.)<br />
FIGURE <strong>144</strong>-8 Seborrheic dermatitis behind the ear in a young<br />
woman. This is a good place to look for evidence of seborrhea. (Courtesy<br />
of Richard P. Usatine, MD.)<br />
FIGURE <strong>144</strong>-9 Seborrhea of the beard and mustache distribution with<br />
prominent erythema. (Courtesy of Richard P. Usatine, MD.)
MHBD125-<strong>144</strong>[615-619].qxd 8/18/08 5:49 PM Page 619<br />
<strong>SEBORRHEIC</strong> <strong>DERMATITIS</strong><br />
10. Vena GA, Micali G, Santoianni P, Cassano N, Peruzzi E. Oral<br />
terbinafine in the t eatment of multi-site seborrhoic dermatitis:<br />
A multicenter, double-blind placebo-controlled study. Int J<br />
Immunopathol Pharmacol. 2005;18:745–753.<br />
11. Scaparro E, Quadri G,Virno G, Orifici , Milani M. Evaluation of<br />
the effica y and tolerability of oral terbinafine (Daskil) in p tients<br />
with seborrhoeic dermatitis.A multicentre, randomized, investigator-blinded,<br />
placebo-controlled trial. Br J Dermatol. 2001;<br />
<strong>144</strong>(4):854–857.<br />
12. Firooz A, Solhpour A, Gorouhi F, et al. Pimecrolimus cream, 1%,<br />
vs hydrocortisone acetate cream, 1%, in the treatment of facial<br />
seborrheic dermatitis:A randomized, investigator-blind, clinical<br />
trial. Arch Dermatol. 2006;142:1066–1067.<br />
13. Freeman SH. Effica y, cutaneous tolerance and cosmetic acceptability<br />
of desonide 0.05% lotion (Desowen) versus vehicle in the<br />
short-term treatment of facial atopic or seborrhoeic dermatitis.<br />
Australas J Dermatol. 2002;43(3):186–189.<br />
14. Rigopoulos D, Ioannides D, Kalogeromitros D, Gregoriou S, Katsambas<br />
A. Pimecrolimus cream 1% vs. betamethasone 17-valerate<br />
0.1% cream in the treatment of seborrhoeic dermatitis.A<br />
randomized open-label clinical trial. Br J Dermatol. 2004;151:<br />
1071–1075.<br />
15. Warshaw EM,Wohlhuter RJ, Liu A, et al. Results of a<br />
randomized, double-blind, vehicle-controlled effica y trial of<br />
pimecrolimus cream 1% for the treatment of moderate to severe<br />
facial seborrheic dermatitis. J Am Acad Dermatol. 2007;57(2):<br />
257–264.<br />
16. Parsad D, Pandhi R, Negi KS, Kumar B.Topical metronidazole in<br />
seborrheic dermatitis—a double-blind study. Dermatology. 2001;<br />
202:35–37.<br />
17. Koca R. Is topical metronidazole effective in seborrheic dermatitis?<br />
A double-blind study. Int J Dermatol. 2003;42(8):632–635.<br />
18. Satchell AC, Saurajen A, Bell C, Barnetson RS.Treatment of dandruff<br />
with 5% tea tree oil shampoo. J Am Acad Dermatol. 2002;<br />
47(6):852–855.<br />
19. Smith SA BAWJ. Effective treatment of seborrheic dermatitis using<br />
a low dose, oral homeopathic medication consisting of potassium<br />
bromide, sodium bromide, nickel sulfate, and sodium chloride<br />
in a double-blind, placebo-controlled study. Altern Med Rev.<br />
2002;7(1):59–67.<br />
PART 13<br />
DERMATOLOGY<br />
619