

Introduction to Ocular Motility Extraocular Muscles EOM ...
Introduction to Ocular Motility Extraocular Muscles EOM ...
Introduction to Ocular Motility Extraocular Muscles EOM ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Introduction</strong> <strong>to</strong> <strong>Ocular</strong> <strong>Motility</strong><br />
Diana J. Shamis, CO, COMT, MHSE<br />
University of Florida<br />
<strong>EOM</strong> Abbreviations<br />
IR - Inferior rectus<br />
SR - Superior rectus<br />
LR - Lateral rectus<br />
MR - Medial rectus<br />
SO - Superior oblique<br />
IO - Inferior oblique<br />
Rectus muscle insertions<br />
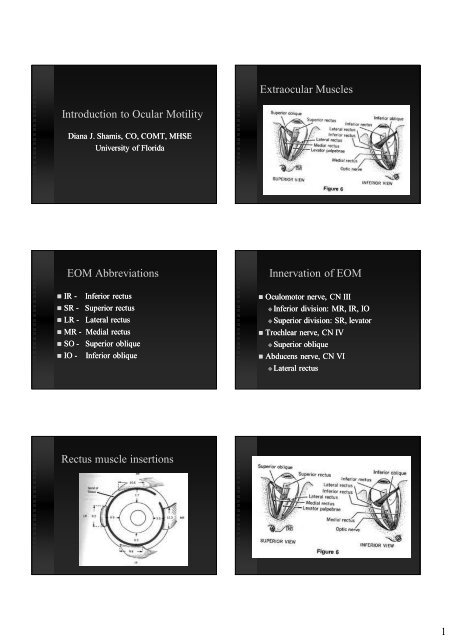
<strong>Extraocular</strong> <strong>Muscles</strong><br />
Innervation of <strong>EOM</strong><br />
Oculomo<strong>to</strong>r nerve, CN III<br />
Inferior Inferior division: MR, IR, IO<br />
Superior Superior division: SR, leva<strong>to</strong>r<br />
Trochlear nerve, CN IV<br />
Superior Superior oblique<br />
Abducens nerve, CN VI<br />
Lateral Lateral rectus<br />
1
Diagnostic Positions of Gaze<br />
2
Ductions and Versions<br />
Versions - Movement of both eyes<br />
Amplitude, smoothness, palpebral fissure<br />
height, pupil size, oscillations.<br />
Ductions – Movement of one eye<br />
If versions abnormal<br />
Improvement on ductions suggests<br />
paretic process<br />
Normal Versions<br />
Normal Versions<br />
Herring’s Law of Equal<br />
Innervation<br />
When an impulse goes <strong>to</strong> a muscle <strong>to</strong><br />
contract, an equal impulse goes <strong>to</strong> it’s<br />
contralateral synergist (yoke muscle).<br />
Sherring<strong>to</strong>n’s Law of<br />
Reciprocal Innervation<br />
When an impulse goes <strong>to</strong> a muscle <strong>to</strong><br />
contract, an equal and opposite<br />
impulse <strong>to</strong> relax goes <strong>to</strong> it’s ipsilateral<br />
antagonist.<br />
CN VI palsy (LR)<br />
Limitation of abduction<br />
3
Brown syndrome<br />
Limited elevation in adduction<br />
SO palsy<br />
Limited depression in adduction<br />
Over-action of IO<br />
Duane - Type I<br />
Incomitant ET due <strong>to</strong> 6th CN palsy.<br />
Abduction deficit <strong>to</strong> the effected side.<br />
Narrowing of the palpebral fissures on adduction of the<br />
effected eye.<br />
CN III palsy<br />
Limited upgaze, downgaze, & adduction<br />
V pattern XT<br />
Recording Under-actions and<br />
Over-actions<br />
50%<br />
70 %<br />
+ 3<br />
-2<br />
4
Vergence<br />
Disconjugate movements of the eyes.<br />
Movement in opposite directions.<br />
Convergence<br />
Convergence – Both eyes turn in<br />
Divergence Divergence – Both eyes turn out<br />
Vertical Vertical vergence – One eye moves up,<br />
the other down<br />
Strabismus<br />
<strong>Ocular</strong> misalignment that prevents bifoveal<br />
fixation.<br />
Non-parallel Non parallel visual axes.<br />
Fixation<br />
Central Fixation<br />
Using Using the fovea <strong>to</strong> fixate<br />
Eccentric Fixation<br />
Using Using a non-foveal non foveal retinal point <strong>to</strong> fixate<br />
Bifoveal fixation<br />
Using Using both foveas <strong>to</strong> fixate the same<br />
object at the same time.<br />
Convergence amplitudes<br />
Measure with base out<br />
prism bar at distance<br />
and near.<br />
Minimum normal<br />
20 prism diopter at<br />
near<br />
12 at distance<br />
Fixation<br />
Maintaining the position of the eye so<br />
that the image of the object of regard<br />
falls on the fovea.<br />
Fovea<br />
Central Fixation<br />
5
Angle Kappa<br />
Heterotropia (Tropia)<br />
Deviation of an eye<br />
which is present under<br />
normal visual<br />
situations.<br />
A “Manifest”<br />
deviation<br />
Not necessarily visible<br />
<strong>to</strong> casual observation.<br />
Heterophoria (Phoria)<br />
Latent tendency for the eyes <strong>to</strong><br />
deviate, which is controlled by fusion.<br />
f<br />
X<br />
f<br />
f<br />
X<br />
X<br />
f<br />
X<br />
f<br />
Eccentric Fixation<br />
Dragged Macula<br />
Heterotropia<br />
Not always apparent <strong>to</strong> casual observation.<br />
Intermittent deviation<br />
A deviation which is sometimes a phoria<br />
and sometimes a tropia.<br />
May vary with position of gaze, distance<br />
from the patient, or fatigue.<br />
6
Intermittent Strabismus<br />
X(T)<br />
Strabismus abbreviations<br />
E – Esophoria ET – Esotropia<br />
X – Exophoria XT – Exotropia<br />
H – Hyperphoria HT – Hypertropia<br />
ht – hypophoria ht – hypotropia<br />
Bracketed (T) indicates intermittent tropia<br />
Ex: X (T) - Intermittent exotropia<br />
Cover- Uncover Test<br />
Detecting a Heterotropia<br />
Differentiating a Tropia from a Phoria<br />
Requires ability <strong>to</strong> fixate with either eye<br />
Alternating Strabismus<br />
Patient alternates which eye is the<br />
straight eye and which eye is deviated.<br />
Detection and Measurement of<br />
Strabismus<br />
Cover - uncover test<br />
Hirschberg corneal reflex test<br />
Krimsky<br />
Prism and alternate cover test<br />
Maddox rod<br />
Cover-Uncover Test<br />
Insure adequate fixation<br />
7
1.<br />
Cover-Uncover Test<br />
Observe eye movement as the<br />
unoccluded eye recovers fixation.<br />
Esotropia Esotropia - Eye pulls out<br />
Exotropia Exotropia - Eye pulls in<br />
Hypertropia Hypertropia - Eye pulls down<br />
Hypotropia Hypotropia - Eye pulls up<br />
Left hypotropia. OD fixing.<br />
3.<br />
Cover-Uncover Cover Uncover Test<br />
Test - Vertical<br />
Vertical<br />
Right Hypertropia. OS fixing.<br />
2.<br />
4.<br />
Cover fixing eye (OD)<br />
Hypotropic OS pulls up.<br />
OD under cover deviates up.<br />
Cover fixing eye (OS)<br />
Hypertropic OD pulls down<br />
OS under cover deviates down<br />
Measuring the deviation<br />
Use PACT if possible<br />
Use Krimsky if patient cannot fixate well.<br />
If only one eye moves - place prism in front of eye<br />
with restricted motion.<br />
1.<br />
3.<br />
Cover-uncover test: Esotropia<br />
LET. OD fixing.<br />
Cover is removed.<br />
Neither eye moves.<br />
Bifovial fixation<br />
2.<br />
4.<br />
Cover deviated OS.<br />
OD does not move.<br />
Cover fixing eye.<br />
Deviated OS pulls out.<br />
OD under cover deviates in.<br />
Cover-uncover test: Exophoria<br />
1. 2.<br />
3.<br />
Cover is removed, deviated<br />
eye moves in <strong>to</strong> regain fusion.<br />
Cover left eye.<br />
Eye under cover deviates out.<br />
Measuring Strabismus<br />
4.<br />
Cover right eye.<br />
Eye under cover deviates out.<br />
PACT - Prism Alternate Cover Test<br />
Most accurate, requires good fixation<br />
Hirschberg and Krimsky<br />
If poor vision, poor fixation, nystagmus<br />
Young children, inattention<br />
Maddox rod<br />
useful for measuring small vertical deviations<br />
in cooperative patient.<br />
8
Hirschberg Corneal Light<br />
Reflex Test<br />
Estimate of deviation by observing<br />
symmetry of corneal light reflexes.<br />
Least accurate means of measurement.<br />
1 mm displacement = 15 <br />
Right Esotropia<br />
Light reflex is out because the eye<br />
is turned in.<br />
Right Hypertropia<br />
Light reflex is down, because the<br />
eye is up.<br />
Hirschberg estimate<br />
Corneal light reflex test<br />
Estimate of deviation<br />
based on amount of<br />
displacement of corneal<br />
light reflex.<br />
1 mm displacement =<br />
15 deviation<br />
30 ET<br />
60 ET<br />
90 ET<br />
Left Exotropia<br />
Light reflex is in, because the<br />
eye is turned out.<br />
Krimsky Prism Reflex<br />
Test<br />
Estimate of the deviation by aligning<br />
the corneal light reflexes with prisms.<br />
Light reflexes should be symmetrical,<br />
not necessarily centered.<br />
9
Krimsky Prism Reflex Test<br />
Prisms are added until light reflexes<br />
are symmetric.<br />
Krimsky: Over-correction<br />
Prism and Alternate Cover Test<br />
Movement of the eyes is neutralized with<br />
prisms.<br />
ET ET– Eye moves out – Base out<br />
XT– XT Eye moves in -Base Base in<br />
HT– HT Eye moves down – Base down<br />
ht - Eye moves up – Base up<br />
Prism position<br />
ET – Light reflex out - Base out<br />
XT – Light reflex in - Base in<br />
HT– HT Light reflex down -Base Base down<br />
ht – Light reflex up -Base Base up<br />
Prism and Alternate Cover Test<br />
Patient must be<br />
able <strong>to</strong> fixate OU.<br />
Cross cover and<br />
add prisms until<br />
motion is<br />
neutralized.<br />
PACT - Esotropia<br />
X<br />
1. 2.<br />
f<br />
X<br />
f<br />
f<br />
3.<br />
X<br />
f<br />
f<br />
X<br />
f<br />
10
X<br />
1. 2.<br />
f<br />
PACT - Exophoria<br />
f<br />
3.<br />
Maddox Rod<br />
Vertical cylinder -<br />
patient sees<br />
horizontal red line.<br />
Use <strong>to</strong> measure HT.<br />
Horizontal cylinders -<br />
patient sees a vertical<br />
red line. Use <strong>to</strong><br />
measure ET or XT.<br />
f<br />
Proper prism position<br />
Parallel <strong>to</strong> floor of the orbit<br />
Perpendicular <strong>to</strong> the line of sight<br />
X<br />
f<br />
f<br />
X<br />
f<br />
Maddox Rod<br />
Patient looks at a light with Maddox Rod over one<br />
eye.<br />
Can not differentiate between phoria and tropia.<br />
Measures latent or manifest deviation.<br />
Maddox rod responses<br />
Maddox Rod over right eye<br />
Ortho Response<br />
Left Hyper<br />
Right Hyper<br />
Exodeviation<br />
Esodeviation<br />
Right gaze - Left gaze<br />
11
Up gaze and Down gaze<br />
Right<br />
Gaze<br />
Recording the Results<br />
PACT, sc: 10 LHT’<br />
10 LHT<br />
15 LHT<br />
5 ET<br />
20 LHT<br />
8 ET<br />
10 LHT<br />
10 LHT<br />
5 ET<br />
10 LHT<br />
8 ET<br />
6 LHT<br />
4 LHT<br />
5 ET<br />
2 LHT<br />
8 ET<br />
4 LHT 15LHT<br />
Childhood Strabismus<br />
Horizontally Comitant Strabismus<br />
Infantile Infantile Esotropia<br />
Accommodative Accommodative Esotropia<br />
Intermittent Intermittent Exotropia<br />
Left<br />
Gaze<br />
Head tilt - right and left<br />
Only needed in HT<br />
Comitant vs. Incomitant<br />
Comitant<br />
Infantile ET<br />
Incomitant<br />
Right LR palsy<br />
60 ET 60 ET 60 ET 45 ET 25 ET OT<br />
Comitant Esotropia<br />
12
Acquired strabismus<br />
Palsies and Restrictions<br />
Incomitant deviations<br />
Deviation Deviation is different in different<br />
positions of gaze.<br />
10 LHT<br />
15 LHT<br />
5 ET<br />
20 LHT<br />
8 ET<br />
10 LHT<br />
10 LHT<br />
5 ET<br />
8 LHT<br />
8 ET<br />
6 LHT<br />
4 LHT<br />
5 ET<br />
2 LHT<br />
8 ET<br />
Incomitant Strabismus<br />
13

