

April 2011: C-15873 Paediatric Optometry Part 1
April 2011: C-15873 Paediatric Optometry Part 1
April 2011: C-15873 Paediatric Optometry Part 1

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Detailed Answers<br />
IMAGE A:<br />
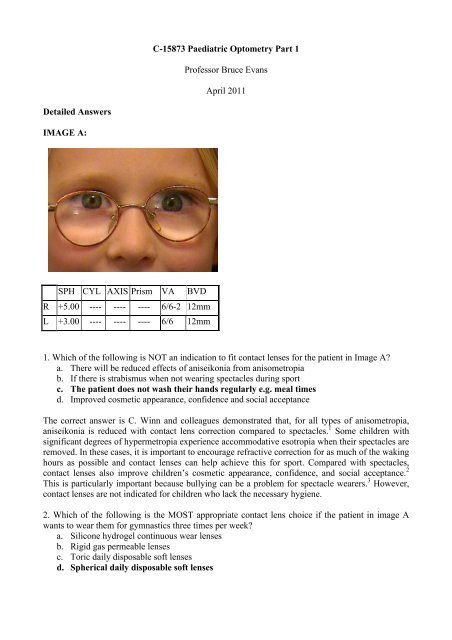
SPH CYL AXIS Prism VA BVD<br />
R +5.00 ---- ---- ---- 6/6-2 12mm<br />
L +3.00 ---- ---- ---- 6/6 12mm<br />
C-<strong>15873</strong> <strong>Paediatric</strong> <strong>Optometry</strong> <strong>Part</strong> 1<br />
Professor Bruce Evans<br />
<strong>April</strong> <strong>2011</strong><br />
1. Which of the following is NOT an indication to fit contact lenses for the patient in Image A?<br />
a. There will be reduced effects of aniseikonia from anisometropia<br />
b. If there is strabismus when not wearing spectacles during sport<br />
c. The patient does not wash their hands regularly e.g. meal times<br />
d. Improved cosmetic appearance, confidence and social acceptance<br />
The correct answer is C. Winn and colleagues demonstrated that, for all types of anisometropia,<br />
aniseikonia is reduced with contact lens correction compared to spectacles. 1 Some children with<br />
significant degrees of hypermetropia experience accommodative esotropia when their spectacles are<br />
removed. In these cases, it is important to encourage refractive correction for as much of the waking<br />
hours as possible and contact lenses can help achieve this for sport. Compared with spectacles,<br />
contact lenses also improve children’s cosmetic appearance, confidence, and social acceptance. 2<br />
This is particularly important because bullying can be a problem for spectacle wearers. 3 However,<br />
contact lenses are not indicated for children who lack the necessary hygiene.<br />
2. Which of the following is the MOST appropriate contact lens choice if the patient in image A<br />
wants to wear them for gymnastics three times per week?<br />
a. Silicone hydrogel continuous wear lenses<br />
b. Rigid gas permeable lenses<br />
c. Toric daily disposable soft lenses<br />
d. Spherical daily disposable soft lenses
The correct answer is D. Spherical lenses (not toric) are appropriate for the prescription shown and<br />
children adapt well to daily disposable lenses which have the advantage of not needing daily<br />
cleaning. 4 Rigid gas permeable lenses are an option, but some children are discouraged by<br />
discomfort during the early stages of adaptation. Continuous wear with silicone hydrogel lenses is<br />
another option, but this modality is fitted less often to children because of the higher risk of<br />
microbial keratitis.<br />
3. When fitting contact lenses for the patient in Image A, which of the following statements is<br />
TRUE?<br />
a. They will accommodate more with spectacles compared to contact lenses<br />
b. They will accommodate less with spectacles compared to contact lenses<br />
c. A correction for back vertex distance is required for the left eye but not the right eye<br />
d. Over-refraction will not be necessary after correction for back vertex distance<br />
The correct answer is A. The ocular accommodation that is required through contact lenses is<br />
different from that through spectacles. Spectacles induce less accommodation in myopes and more<br />
accommodation in hyperopes than that exerted by an emmetrope, or the ametrope when wearing<br />
contact lenses. A correction for back vertex distance is most important in the more hypermetropic<br />
eye. But even if such a correction is made the patient should still be over-refracted to check the<br />
optimal power for contact lenses.<br />
IMAGE B:<br />
SPH CYL AXIS Prism VA BVD<br />
R +5.50 -0.25 180 ---- 6/6 12mm<br />
L +5.00 ---- ---- ---- 6/6 12mm<br />
4. What is the CORRECT description for the binocular vision anomaly shown in Image B?<br />
a. Superior oblique palsy<br />
b. Fully accommodative esotropia<br />
c. Divergence weakness esotropia<br />
d. Convergence weakness exotropia<br />
The correct answer is B. The photographs show a right esotropia without spectacles, which is<br />
straightened by refractive correction. This is a fully accommodative esotropia. 5<br />
5. What is the CORRECT description for the refractive condition shown in Image B?<br />
a. Anisometropic hypermetropia<br />
b. Symmetrical hypermetropia<br />
c. Pseudo over-accommodation
d. All the above<br />
The correct answer is B. The prescription shows hypermetropia that is similar in each eye. This is<br />
therefore symmetrical hypermetropia.<br />
6. What is the MOST appropriate management option for the patient in Image B?<br />
a. Use of spectacles only for near concentrated work<br />
b. Full time wear of spectacles or contact lenses<br />
c. Strabismus surgery<br />
d. All the above<br />
The correct answer is B. For accommodative esotropia, which is eliminated when the<br />
hypermetropia is corrected, the only management is refractive correction. With this degree of<br />
hypermetropia the patient is likely to need spectacles for distance vision as well as near, which will<br />
help to prevent strabismus at distance. Strabismus surgery would be the wrong option. This is<br />
because even if surgery could straighten the visual axes in childhood, then later when the<br />
hypermetropia needed correction because accommodation reduces with age, refractive correction<br />
could cause a secondary exotropia.<br />
IMAGE C: Reproduced with kind permission from Professor David Thomson (Thomson Software<br />
Solutions’ Test Chart 2000 Pro)<br />
I II<br />
III IV<br />
7. A four-year-old patient attends for their first eye examination. Which of the charts shown in<br />
Image C is the LEAST appropriate to use?<br />
a. PANEL I<br />
b. PANEL II<br />
c. PANEL III<br />
d. PANEL IV<br />
The correct answer is D. an isolated optotype is the least appropriate target to use. One of the main<br />
purposes of testing visual acuity in children is to detect strabismic amblyopia, which is most likely<br />
to be detected if crowded rather than single optotypes are used. 5 Generally, it is better to use letters<br />
that have been matched for legibility rather than pictures, but crowding is such an important factor<br />
that it is probably preferable to use crowded pictures in preference to isolated letters.
8. Which one of the following is an advantage of the chart design shown in PANEL I of Image C?<br />
a. The spacing of the optotypes and the lines follows a geometric progression<br />
b. The same number of optotypes are presented on each line<br />
c. There are equal crowding affects on each of the lines of acuity<br />
d. All the above<br />
The correct answer is D. Panel I shows a Bailey-Lovie design of letter chart. 6 Compared with<br />
Snellen charts, the Bailey-Lovie design has several important advantages including the letter size<br />
and inter-letter and inter-line spacing progress logarithmically from one line to the next and the<br />
same number of optotypes are presented on each line. These features mean that there are similar<br />
crowding effects and task difficulty on each line.<br />
9. Which one of the following differences in chart design between the charts shown in PANEL I of<br />
Image C and PANEL II of Image C is TRUE?<br />
a. The optotypes in PANEL I are 5x4 in size whilst the optotypes in PANEL II are 5x5 in<br />
size<br />
b. The optotypes in PANEL I follow a logarithmic progression whilst the optotypes in PANEL<br />
II follow an arithmetic progression<br />
c. The optotypes in PANEL I have less crowding effects than the optotypes in PANEL II<br />
d. The optotypes in PANEL I are suitable for children under the age of 4 years<br />
The correct answer is A. The Bailey-Lovie chart uses letters that are slightly narrower than they are<br />
tall (5x4) whereas the Kay pictures are 5x5 in dimensions, following the Sloan design. The<br />
optotypes in both Panel I and Panel II follow a logarithmic progression and should induce similar<br />
crowding effects although a casual inspection might suggest less inter-optotype spacing in panel I,<br />
which could result in more crowding. It is easier to standardise the legibility of letters than pictures,<br />
although pictures like the Kay ones or the Lea pictures (not show) may be necessary for some<br />
children under the age of 4 years.<br />
IMAGE D:<br />
10. Which one of the following statements about the condition shown in Image D is FALSE?<br />
a. This could be a congenital cataract<br />
b. This could be retinoblastoma<br />
c. This could be bilateral myopia<br />
d. This could be a persistent pupillary hyperplastic vitreous<br />
The correct answer is C. A white pupil (leukocoria) should always be taken seriously, although<br />
sometimes a dilated fundoscopy shows this to be a false alarm. A true white pupil, like that shown<br />
in the image, could have several causes, including congenital cataract, persistent pupillary<br />
hyperplastic vitreous, retinal detachment, or of most concern retinoblastoma. Assuming that the<br />
child is fixating the camera properly, it is not likely to be bilateral myopia.<br />
11. What is the MOST appropriate management for the condition shown in Image D?<br />
a. No management is required, review in 6 months<br />
b. No management is required, review in 1 year<br />
c. Routine referral to ophthalmology is required
d. Prompt referral to ophthalmology is required<br />
The correct answer is D. Since there is a risk of retinoblastoma, a rapid referral is indicated. Even if<br />
it is a less serious condition than retinoblastoma, like congenital cataract, then surgery as young as<br />
possible will increase the probability of some usable acuity in this eye. 7<br />
12. If the condition shown in Image D is corrected with phacoemulsification surgery, what is the<br />
MOST likely management to be undertaken following surgery?<br />
a. Refractive correction with occlusion of the operated eye<br />
b. Refractive correction with occlusion of the good eye<br />
c. Refractive correction without occlusion<br />
d. No further management will be undertaken<br />
The correct answer is B. If the white pupil is the result of a cataract then, even if early surgery takes<br />
place, there is still likely to be dense deprivation amblyopia. If an intraocular implant is not used,<br />
then the child will need contact lenses and occlusion. Even if an intraocular implant is used, then<br />
there is still likely to be a residual refractive error so that the most likely outcome is refractive<br />
correction and occlusion of the good eye.














