

Precocious Pseudopuberty With Testicular Enlargement - medIND
Precocious Pseudopuberty With Testicular Enlargement - medIND
Precocious Pseudopuberty With Testicular Enlargement - medIND

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Clinical Brief<br />
<strong>Precocious</strong> <strong>Pseudopuberty</strong> <strong>With</strong> <strong>Testicular</strong> <strong>Enlargement</strong><br />
R. Rajput, A. Bhansali, R. Bhat and R. Sialy<br />
Department of Endocrinology, Postgraduate Institute of Medical Education and Research, Chandigarh, India<br />
Abstract. Gonadotropins independent precocious puberty (GIPP) in male is characterized by early appearance of sexual hairs<br />
and phallic growth but without testicular enlargement. We report a case of GIPP with testicular enlargement who was diagnosed<br />
to have testotoxicosis and successfully managed with spironolactone. [Indian J Pediatr 2006; 73 (4) : 356-358]<br />
E-mail : anilbhansali_endocrine@rediffmail.com<br />
Key words : <strong>Precocious</strong> pseudopuberty; Testotoxicosis<br />
Puberty is the process of physical maturation manifested<br />
by an increase in growth rate and appearance of<br />
secondary sexual characteristics. Puberty is said to be<br />
precocious if it occurs in boys younger than 9 years of age,<br />
while in girls, less than 7 years of age, and in African<br />
American girls younger than 6 years of age. 1 <strong>Precocious</strong><br />
puberty can be divided into two categories. The first<br />
category is gonadotropins dependent precocious puberty<br />
(GDPP) or true precocious puberty, which involves the<br />
premature activation of hypothalamic-pituitary-gonadal<br />
axis and characterized by appearance of axillary and<br />
pubic hairs along with testicular enlargement. The second<br />
category is gonadotropins independent precocious<br />
puberty (GIPP) or precocious pseudopuberty in which the<br />
increase in sex steroids is independent of pituitary<br />
gonadotropins release, and axillary and pubic hairs<br />
appear along with phallic enlargement but without<br />
associated testicular enlargement.<br />
We describe a case of a five and a half year old boy<br />
who presented with precocious pseudopuberty with<br />
testicular enlargement.<br />
Correspondence and Reprint requests : Dr. Anil Bhansali,<br />
Department of Endocrinology, Postgraduate Institute of Medical,<br />
Education and Research, Chandigarh- 160012, India. Fax : 91-172-<br />
744401, 745078<br />
1, 2<br />
CASE REPORT<br />
A five and a half-year-old boy presented with progressive<br />
phallic enlargement, development of axillary and pubic<br />
hairs, aggressive behavior and rapid increase in height<br />
over the last two years. The child was born of a nonconsanguineous<br />
marriage and had no family history of<br />
precocious puberty. He had no history of central nervous<br />
system infections, head injury, neoplasm or prior<br />
radiation and exposure to exogenous sex steroids. On<br />
examination, his height was 128 cm (90 th percentile) and<br />
weight was 23.4 kg, with target height of 165.3cm. He had<br />
no café-au-lait spots and bony swellings. Systemic<br />
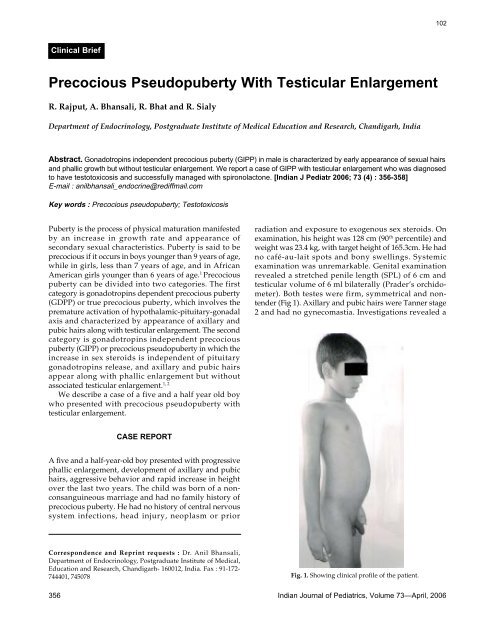
examination was unremarkable. Genital examination<br />
revealed a stretched penile length (SPL) of 6 cm and<br />
testicular volume of 6 ml bilaterally (Prader’s orchidometer).<br />
Both testes were firm, symmetrical and nontender<br />
(Fig 1). Axillary and pubic hairs were Tanner stage<br />
2 and had no gynecomastia. Investigations revealed a<br />
Fig. 1. Showing clinical profile of the patient.<br />
356 Indian Journal of Pediatrics, Volume 73—April, 2006<br />
102
103<br />
bone age of 10 years. Basal serum lentiaisling hormone<br />
(LH) was
Pediatric Endocrine Society. Pediatrics 1999; 104 : 936-941.<br />
2. Marke DP, Cutler GB Jr. Evaluation and management of<br />
<strong>Precocious</strong> puberty. Arch Dis Child 1996: 296-371.<br />
3. Low LC, Wang Q: Gonadotropin indepaendent precocious<br />
puberty. J Pediatr Endocrinol Metab 1998: 497-507.<br />
4. Melvin M Grumbach, Dennis M Styne. Puberty: Ontogeny,<br />
meuroendocronology, physiology and disorders. In Larsen,<br />
Kronenberg, Metmed, polonsky, eds. Williams’s textbook of<br />
Endocrinology. Phialdelphia; WB Saunders, 2003; 1219-1221.<br />
5. Egli CA, Rosenthal SM, Grumbach MM et al. Pituitiary<br />
gonadotropin-independent male-limited autosomal domonant<br />
sexual precocity in nine generations: familial testotoxicosis.<br />
R. Rajput et al<br />
Arch Pathol Lab Med 1985; 109 : 990-995.<br />
6. Shenker A, Laue L, kosugi S et al. A constitutively activating<br />
mutation of the luteinizing hormone receptor in familial male<br />
precocious puberty. Nature 1993; 365: 652-654.<br />
7. Laue L, Kenigsberg D, Pescovitz OH. Treatment of familial<br />
male precocious puberty with spironolactone and testolactone.<br />
N Engl J Med 1989; 320 : 498-502.<br />
8. Leschek EW, Jones J, Barnes KM et al. Six year results of<br />
spironolactone ans testolactone treatment of familial malelimited<br />
precocious puberty with addition of deslorelin after<br />
central puberty onset. J Clin Endocrinol Metab 1999; 84(1) : 175-<br />
178.<br />
358 Indian Journal of Pediatrics, Volume 73—April, 2006<br />
104














