7. Bremer MR-Workschop Tipps und Tricks Männliches Becken
7. Bremer MR-Workschop Tipps und Tricks Männliches Becken
7. Bremer MR-Workschop Tipps und Tricks Männliches Becken
- TAGS
- bremer
- tipps
- tricks
- becken
- www.zemodi.de

Erfolgreiche ePaper selbst erstellen
Machen Sie aus Ihren PDF Publikationen ein blätterbares Flipbook mit unserer einzigartigen Google optimierten e-Paper Software.
<strong>7.</strong> <strong>Bremer</strong> <strong>MR</strong>-<strong>Workschop</strong><br />
<strong>Tipps</strong> <strong>und</strong> <strong>Tricks</strong><br />
<strong>Männliches</strong> <strong>Becken</strong><br />
Wassilios Pegios<br />
Universitätsspital Basel, Institut für Diagnostische Radiologie
•<br />
•<br />
•<br />
•<br />
Kleines <strong>Becken</strong><br />
Primärdiagnostik <strong>und</strong> Nachsorge<br />
Hohe Ortsauflösung / hoher Weichteilkontrast (Fett, Muskel,<br />
<strong>Becken</strong>organe), Bewegungsartefakte<br />
Deutlich verbesserte Sensitivität durch moderne Spulen &<br />
Gradienten, Spektroskopie, Kontrastmittel-Dynamik <strong>und</strong><br />
Sequenzwichtung<br />
Statische <strong>und</strong> dynamische Untersuchungen in einer Sitzung<br />
(Tumorstaging, <strong>MR</strong>-Defäkogr., HSG-<strong>MR</strong>I)<br />
Möglichkeit der Anwendung von spezifischen Kontrastmitteln<br />
(Vasovist, Sinerem, HSG-Dotarem)
Themen<br />
• Fortschritte der <strong>MR</strong>-Technologie<br />
• Prostata<br />
• Harnblase<br />
• Darm: Rektum<br />
• Analkanal (Fisteln, Defäkographie)
• Oberflächenspulen<br />
• Endorektalspulen<br />
• Mehrkanal-Technologie<br />
<strong>MR</strong>-Technologie<br />
• Integrierte Parallele Bildgebung<br />
(iPAT)
Magnete<br />
<strong>MR</strong>-Technologie<br />
Gradienten<br />
80´er 90´er Heute<br />
Empfangsspulen
Qualität<br />
lokale <strong>MR</strong>T<br />
LP<br />
Coils<br />
Gewinn an<br />
SNR (40%)<br />
CP<br />
Coils<br />
<strong>MR</strong>-Technologie<br />
Integrierte Parallele Bildgebung (iPAT)<br />
Vergr. FOV<br />
Kombination<br />
mehrerer CP-Spulen<br />
CP<br />
Array<br />
IP<br />
Array<br />
Ganzkörper-<br />
<strong>MR</strong>T<br />
Matrix<br />
Coils<br />
1983 1988 1993 1997 2003<br />
linear polarization<br />
circular polarization<br />
Array-Spulen:<br />
verbesserte<br />
Bildfeldhomogenität<br />
im FOV <strong>und</strong> höchstes<br />
SNR<br />
Zeit
<strong>MR</strong>-Technologie<br />
Dr. Damadian 1977 1.5 Tesla whole-body <strong>MR</strong>I, 2003
• Keine Darmvorbereitung<br />
• Endorektalspule<br />
• Buscopan<br />
Prostata<br />
Localizer<br />
T2TSE tra, cor SD 3mm<br />
(ca. 7:00)<br />
Voxel: (0,8 x 0,4 x 3,0) mm3 T1TSE tra SD 3/0,3 mm (ca. 3:20)<br />
Voxel: (1,3x1,0x3,0) mm3 <strong>MR</strong>-Spektroskopie<br />
(TR/TE:650/120 ms; 6x6x6 mm<br />
(ca. 10:00)<br />
3 )<br />
KM-Dynamik tra VIBE<br />
(ca. 5-6:00)
Prostata-Ca<br />
T2-TSE, trans T2-TSE, cor
Prostata<br />
► Treffsicherheit beim lokalen Staging:<br />
Sens. / Spez.= 80%-95% / 82%-93%<br />
Treffsicherheit 82-88%<br />
•Tumorlokalisation<br />
Sens. / Spez. = ca. 80% - 50%<br />
•extrakapsuläre Ausbreitung<br />
Sens. / Spez. = ca. 85% -80%<br />
•Samenblaseninfiltration<br />
Sens. / Spez. = ca. 80% - 95%<br />
► Hinweis für Kosteneffizienz<br />
Engelbrecht <strong>MR</strong>, et al.<br />
Eur Radiol 2002; 12:2294<br />
Heuck A et al.<br />
Radiologe 2003; 43:464<br />
Jager et al.<br />
Radiology 2000; 215:445<br />
Schlemmer et al.<br />
Eur Radiol 2004; 14:309<br />
Eur Radiol 2004; 14:597
Prostata: Limitationen<br />
► BPH<br />
► Prostatitis<br />
► Granulomatöse Prostatitis<br />
► PIN<br />
► Fibrose<br />
► Hämorrhagien<br />
► Antihormonelle Therapie
Problem<br />
•Die <strong>MR</strong>T erreicht bei der Tumordetektion eine höhere Sensitivität<br />
(83%) als die DRU <strong>und</strong> der TRUS. Die Spezifität ist jedoch gering<br />
(62%), da andere Bef<strong>und</strong>e wie PIN, Prostatitis, Fibrosen oder<br />
Hämorrhagien ähnliche Veränderungen bewirken.<br />
•Der Einsatz zusätzlicher Techniken wie KM-unterstützte<br />
dynamische <strong>MR</strong>T <strong>und</strong> <strong>MR</strong>-Spektroskopie lassen die Sensitivität<br />
<strong>und</strong> insbesondere die Spezifität der Tumordetektion verbessern.<br />
•Die erste durch TRUS gesteuerte Prostatabiopsie trotz suspekte<br />
PSA-Werte bis zu 66 -71 % negativ.<br />
•Zur Lösung dieses Dilemmas wurden bisher eine<br />
Verlaufskontrolle des PSA-Werts <strong>und</strong> gegebenfalls eine<br />
Wiederholung der Biopsie möglicherweise mit einer vergrösserten<br />
Anzahl an Biopsien vorgeschlagen.
DCE - <strong>MR</strong>T<br />
T2-TSE axial <strong>und</strong> koronar:<br />
• konfluierende signalarme Areale in der peripheren Zone<br />
werden als tumorsuspekt eingestuft<br />
• diffuse <strong>und</strong> inhomogen signalarme Areale werden als nicht<br />
eindeutig tumorsuspekt eingestuft<br />
KM-Dynamik:<br />
• Analyse der Anstiegsgeschwindigkeit <strong>und</strong> max.<br />
Signalintensität<br />
• Signalintensitätsgipfel innerhalb der ersten 2 Minuten<br />
• „Auswaschphänomen“ 1<br />
• Relatives maximales Enhancement (vom max. Enhancement<br />
imTumor wird das durchschnittliche Enhancement von<br />
umliegenden Gewebe abgezogen) 2<br />
1 Padhani AR, et al.: Effects of androgen deprivation on prostatic morphology and vascular permeability evaluated with<br />
<strong>MR</strong> imaging. Radiology 2001;218:365-374<br />
2 Engelbrecht <strong>MR</strong>, et al.: Discrimination of prostate cancer from normal peripheral zone and central gland tissue by using<br />
dynamic contrast-enhanced <strong>MR</strong> imaging. Radiology 2003;229:248-254
Model of Contrast kinetics in Tumors<br />
Cellular density (“Extracellular Volume Fraction”)<br />
Blood vessel permeability (“Vascular Permeability”)<br />
Blood<br />
Renal<br />
Elimination<br />
Body<br />
Compartments<br />
Prostate<br />
Cancer<br />
EVF<br />
PERM<br />
Benign Lesions Malignant Tumors<br />
= EVF<br />
= PERM
Vascular Permeability<br />
Cancer<br />
Pharmacokinetic Analysis of DCE-<strong>MR</strong>I<br />
Full Analysis<br />
Option<br />
Extracellular Space<br />
Benign<br />
Contrast<br />
Injection<br />
EC Space Tumor<br />
Blood Volume<br />
Tumor<br />
Blood Circulation<br />
Blood Volume<br />
Body<br />
Vascular Permeability<br />
Vascular Permeability<br />
Renal<br />
Elimination<br />
Extracellular Space<br />
C<br />
B<br />
Quick 3TP<br />
Option
T2-TSE-Sequenz<br />
Dynamik, VIBE-Sequenz<br />
„time-to-peak“
Full Analysis of DCE-<strong>MR</strong>I<br />
DCE <strong>MR</strong>I<br />
pre contrast<br />
DCE <strong>MR</strong>I<br />
LATE post contrast<br />
Staging<br />
DCE <strong>MR</strong>I<br />
EARLY post contrast<br />
DCE <strong>MR</strong>I 3TP-MAP
DCE <strong>MR</strong>I<br />
pre contrast<br />
DCE <strong>MR</strong>I<br />
LATE post contrast<br />
Full Analysis of DCE-<strong>MR</strong>I<br />
Prostate Cancer Detection<br />
Elevated PSA - neg. Biopsy<br />
DCE <strong>MR</strong>I<br />
EARLY post contrast<br />
DCE <strong>MR</strong>I 3TP-MAP
Fallbeispiele<br />
Karzinom<br />
BPH-Knoten
ges<strong>und</strong>es Prostatagewebe<br />
Cho<br />
Cit<br />
1 H-<strong>MR</strong>-Spektroskopie<br />
3D- Chemical Shift Imaging (CSI)<br />
Prostatakarzinom<br />
Cho<br />
Cit
Position des 3D CSI Volumens<br />
1 H-<strong>MR</strong>-Spektroskopie<br />
3D- Chemical Shift Imaging (CSI)<br />
Messvolumen<br />
16 x 16 Grid<br />
örtliche Zuordnung
1 H-<strong>MR</strong>-Spektroskopie<br />
3D- Chemical Shift Imaging (CSI)<br />
erhöhtes Cho<br />
Metabolitenbild
Diffusions-gewichtete Sequenzen<br />
T2-TSE DWI<br />
DCE<br />
DCE<br />
ADC<br />
Tanimoto A et al.:<br />
Prostate cancer screening: the clinical value of diffusion-weighted imaging and dynamic <strong>MR</strong> imaging in<br />
combination with T2-weighted imaging. J Magn Reson Imaging 2007 Jan; 25 (1) :146-152
T2 T2<br />
DCE <strong>MR</strong>I 3TP-MAP<br />
DWI ADC DWI ADC
<strong>MR</strong>-gesteuerte Biopsie
<strong>MR</strong>-gesteuerte Biopsie<br />
Blumenfeld Ph. et al.:<br />
Transperineal prostate biopsy <strong>und</strong>er magnetic resonance image guidance:<br />
A needle placement accuracy study. J Magn Reson Imaging 2007 Sep;26(3):688-94
Prostata-Ca: Stadium T4N1<br />
T2-TSE<br />
cor<br />
ax sag
LK-spezifische KM: “Sinerem”
LK-spezifische KM: “Sinerem”
3 Tesla, Oberflächenspule<br />
T2 DWI<br />
T2 DWI<br />
Miao H et al.:<br />
Prostate cancer detection with 3-T <strong>MR</strong>I: comparison of diffusion-weighted and T2-weighted imaging.<br />
Eur J Radiol. 2007 Feb;61(2):297-302
•<br />
•<br />
Gefüllte Harnblase<br />
1-2 Amp. Buscopan<br />
Harnblase<br />
i.v.<br />
Localizer<br />
T2 TSE tra, cor, sag<br />
SD 4 mm (ca. 10:00)<br />
T1 TSE tra (gesamtes <strong>Becken</strong>) SD 4 mm (3:46)<br />
T1 VIBE vor/nach i.v. KM<br />
isotope Voxel: (1,1mm<br />
(1:46)<br />
3 )<br />
[SPACE (8-10:00)]
T2-w<br />
Harnblasen-Ca<br />
T1-VIBE<br />
T2b<br />
T1
Harnblasen-Ca<br />
Diffusions-gewichtete <strong>MR</strong>T<br />
T2-w DWI ADC<br />
TR/TE: 4900-8000 / 68 ms<br />
SD: 5mm, 128 x 128 Matrix<br />
FOV: 480
•<br />
•<br />
•<br />
Keine Abführmassnahmen<br />
Ca. 200 ml US-Gel rektal<br />
1-2 Amp. Buscopan i.v.<br />
Localizer (TRUFI oder Haste)<br />
Rektum<br />
T2TSE sag, oblique ax (SD 4mm) (ca. 7:00)<br />
T1TSE ax (gesamtes <strong>Becken</strong>, 4mm) (ca. 3:46)<br />
T1VIBE vor/nach KM (ca. 1:46)<br />
isotope<br />
Voxel: (1,1mm 3 )<br />
[SPACE 8-10:00]
T2-haste-bh<br />
TR / TE: 1110 / 102<br />
Rektumkarzinom<br />
T1-fl3D-fs-bh-vibe<br />
TR / TE: 3.1 / 1.2
•<br />
•<br />
•<br />
•<br />
Spikulationen<br />
-desmoplastische<br />
-radiogene<br />
-<br />
Noduläre<br />
-hohe<br />
Rektumkarzinom<br />
im mesorektalen<br />
Fibrose<br />
BG-Reaktionen +/-<br />
+/-<br />
Fettgewebe hervorgerufen durch:<br />
Tumorzellen<br />
Tumorzellen<br />
geringer Vorhersagewert: PPV = 65%<br />
Veränderungen jenseits der Rektumwand:<br />
Aussagekraft: PPV = 98%<br />
Geringe Genauigkeit hinsichtlich anteriorer Tumorausdehnung<br />
wegen Kompression der Organe (Vagina, Prostata, SB)<br />
CE-T1-TSE ohne Vorteil gegenüber T2w-TSE (Accuracy<br />
90%)
Rektum-Ca: T2 vs. T3<br />
T2 T3 T3<br />
Vliegen R et al.:<br />
Rectal Cancer: <strong>MR</strong> Imaging in Local Staging-Is Gadolinium-based Contrast Material Helpful?<br />
Radiology 2005;234:179-188
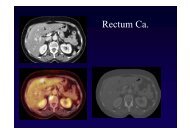
Rektum-Ca / Leberfiliae
T2-TSE<br />
Rektumkarzinom<br />
Prä- <strong>und</strong> posttherapeutisches Staging<br />
Vor Therapie Nach Therapie
3 Tesla, Oberflächenspule
•<br />
•<br />
•<br />
Phase-Array-Coil<br />
Endorektalspule<br />
Buscopan i.v.<br />
Localizer (TRUFI oder Haste)<br />
Analkanal<br />
T2-TSE-FS ax, sag, cor (SD 3/0.3) (4:46)<br />
T1TSE ax (4:19)<br />
T1-TSE-FS ax, cor, sag nach KM (5:55)<br />
[SPACE 8-10:00]
Anal-Sphinkter<br />
Anal Sphinkter-Komplex Komplex: : ES<br />
Normale Anatomie
Anal-Sphinkter<br />
Anal Sphinkter-Komplex Komplex: : Fisteln
Analfisteln: Body-Phased-Array<br />
Hufeisenfistel<br />
T2-TSE cor
Analkanal: Body-Phased-Array<br />
Analfistel<br />
T2-TSE-FS<br />
ax cor<br />
T1-TSE-FS<br />
post-KM
Current<br />
•Defecatory<br />
(established) clinical<br />
disorders<br />
Obstipation<br />
Fecal<br />
Obstructed<br />
Anismus<br />
•Suspectet<br />
<strong>MR</strong>-DEFECOGRAPHY<br />
<strong>MR</strong> DEFECOGRAPHY<br />
incontinence<br />
defacation<br />
(spastic<br />
descending<br />
pelvic<br />
indications<br />
floor<br />
perineum<br />
syndrome)<br />
syndrome
DYNAMIC PELVIC FLOOR <strong>MR</strong>I<br />
•Visualizes<br />
pelvic<br />
floor<br />
motion<br />
in realtime<br />
•Alternative to fluoroscopic techniques (i.e. evacuation<br />
proctography) but with lack of irradiation and inherent soft<br />
tissue contrast<br />
at rest max.<br />
contraction<br />
straining
Normale Anatomie
Patient Preparation<br />
•No oral bowel<br />
•Bladder<br />
<strong>MR</strong>-DEFECOGRAPHY<br />
<strong>MR</strong> DEFECOGRAPHY<br />
should<br />
preparetion<br />
be<br />
full<br />
•Allways: Rectal filling with ultraso<strong>und</strong><br />
patatoes (300 ml @ 1.5 ml Gd)<br />
•On demand: Vaginal filling<br />
filling of the bladder<br />
with<br />
gel<br />
ultraso<strong>und</strong><br />
Healy JC et al. AJR 1997; 169:775; Gufler H et al. J<strong>MR</strong>I 1999; 9:378;<br />
Kelvin FM et al. AJR 2000; 174:81; Unterweger<br />
(300 ml) or<br />
M et al. AJR 2001; 176: 959<br />
mashed<br />
gel; retrograde
•Phased-array-pelvic coil<br />
•Bildgebung in sagittaler Ebene<br />
Sequenz TR<br />
(ms)<br />
TE<br />
(ms)<br />
Protokoll<br />
FoV SD<br />
(mm)<br />
Matrix Orient. Dauer<br />
(m/s)<br />
T2-TSE (nativ) 4830 115 180*180 5 204*256 ax, sag 3:15<br />
T1-TSE (nativ) 660 11 200*200 5 272*320 ax 3:34<br />
T2-trufi-dyn<br />
Ruhe-Kontraktion<br />
T2-trufi-dyn<br />
Ruhe-Pressen<br />
Defäkation<br />
Post 10s Defäkation<br />
Schlussbilder<br />
Gel-Füllung rektal<br />
3.4 1.1 255*340 5 173*256 sag 0:13<br />
330 2 250*250 10 256*256 sag 0:36
Anterior<br />
Compartiment<br />
Cystocele<br />
Pathologische Landmarken<br />
Middle Compartiment<br />
Vaginal vault descent<br />
Posterior<br />
Compartiment<br />
Rectocele<br />
Rectal<br />
Descent<br />
Intussusception<br />
Anismus
RECTOCELE<br />
small anterior rectocele moderately sized anterior rectocele
Intussuszeption<br />
58-jährige Patientin. Stuhlschmieren. Rektozelle?
Bladder / Vaginal vault descent<br />
Descent of the bladder base<br />
the pubococcygeal line (PL)<br />
Small: < 3 cm below<br />
Moderate: between<br />
below PL<br />
Large: > 6 cm below<br />
PL<br />
3 and 6 cm<br />
PL<br />
below
Grading of <strong>MR</strong> Imaging Findings<br />
*Below<br />
the<br />
Intussusceptions<br />
inferior pubococcygeal<br />
were<br />
not<br />
graded<br />
line<br />
Bertschinger et al.: Dynamic <strong>MR</strong> Imaging of the Pelvic Floor Performed with Patient Sitting in an Open-<br />
Magnet Unit versus with Patient Supine in a Closed-Magnet Unit. Radiology 2002; 223:501-508
69-jährige Patientin<br />
progredientes<br />
Stuhlschmieren<br />
klinisch V.a. Sphinkterdefekt<br />
<strong>und</strong> ventrale Rektozelle<br />
<strong>Becken</strong>bodendysfunktion<br />
kleine anteriore Rektozelle
Verbesserungen:<br />
•Diagnostik (u.a. 3D-<br />
Datensätze)<br />
•Untersuchungszeiten<br />
•Zufriedenheit von<br />
Patient <strong>und</strong> Zuweiser<br />
Ausblick<br />
Probleme:<br />
•Handhabung der<br />
komplexen Daten<br />
•Erfahrung des<br />
Untersuchers<br />
•Zeitaufwändige <strong>und</strong><br />
interaktive Bef<strong>und</strong>ung<br />
•inadäquate Vergütung<br />
komplexer<br />
Untersuchungen<br />
Effektivität / Workflow<br />
?
Vielen Dank für Ihre<br />
Aufmerksamkeit!