

spektrum der augenheilkunde - 150 Jahre Augenklinik Graz
spektrum der augenheilkunde - 150 Jahre Augenklinik Graz
spektrum der augenheilkunde - 150 Jahre Augenklinik Graz

Sie wollen auch ein ePaper? Erhöhen Sie die Reichweite Ihrer Titel.
YUMPU macht aus Druck-PDFs automatisch weboptimierte ePaper, die Google liebt.
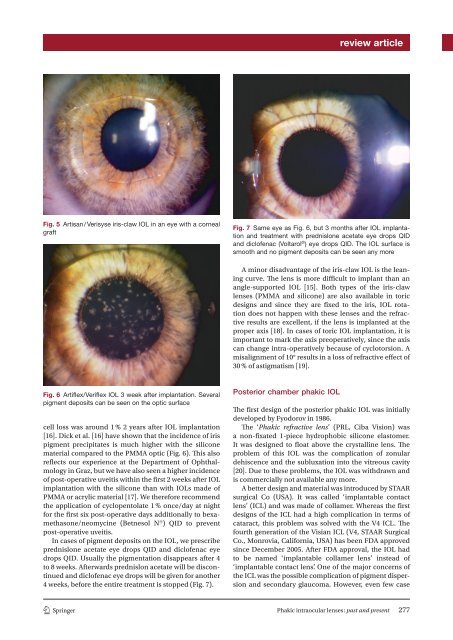
eview articleFig. 5 Artisan / Verisyse iris-claw IOL in an eye with a cornealgraftFig. 7 Same eye as Fig. 6 , but 3 months after IOL implantationand treatment with prednislone acetate eye drops QIDand diclofenac (Voltarol ® ) eye drops QID. The IOL surface issmooth and no pigment deposits can be seen any moreA minor disadvantage of the iris-claw IOL is the leaningcurve. The lens is more difficult to implant than anangle-supported IOL [ 15 ]. Both types of the iris-clawlenses (PMMA and silicone) are also available in toricdesigns and since they are fixed to the iris, IOL rotationdoes not happen with these lenses and the refractiveresults are excellent, if the lens is implanted at theproper axis [ 18 ]. In cases of toric IOL implantation, it isimportant to mark the axis preoperatively, since the axiscan change intra-operatively because of cyclotorsion. Amisalignment of 10° results in a loss of refractive effect of30 % of astigmatism [19 ].Fig. 6 Artiflex/Veriflex IOL 3 week after implantation. Severalpigment deposits can be seen on the optic surfacecell loss was around 1 % 2 years after IOL implantation[ 16 ]. Dick et al. [ 16 ] have shown that the incidence of irispigment precipitates is much higher with the siliconematerial compared to the PMMA optic (Fig. 6 ). This alsoreflects our experience at the Department of Ophthalmologyin <strong>Graz</strong>, but we have also seen a higher incidenceof post-operative uveitis within the first 2 weeks after IOLimplantation with the silicone than with IOLs made ofPMMA or acrylic material [ 17 ]. We therefore recommendthe application of cyclopentolate 1 % once/day at nightfor the first six post-operative days additionally to bexamethasone/neomycine(Betnesol N ® ) QID to preventpost-operative uveitis.In cases of pigment deposits on the IOL, we prescribeprednislone acetate eye drops QID and diclofenac eyedrops QID. Usually the pigmentation disappears after 4to 8 weeks. Afterwards prednislon acetate will be discontinuedand diclofenac eye drops will be given for another4 weeks, before the entire treatment is stopped (Fig. 7 ).Posterior chamber phakic IOLTh e first design of the posterior phakic IOL was initiallydeveloped by Fyodorov in 1986.Th e ‘ Phakic refractive lens ’ (PRL, Ciba Vision) wasa non-fixated 1-piece hydrophobic silicone elastomer.It was designed to float above the crystalline lens. Theproblem of this IOL was the complication of zonulardehiscence and the subluxation into the vitreous cavity[ 20 ]. Due to these problems, the IOL was withdrawn andis commercially not available any more.A better design and material was introduced by STAARsurgical Co (USA). It was called ‘implantable contactlens’ (ICL) and was made of collamer. Whereas the firstdesigns of the ICL had a high complication in terms ofcataract, this problem was solved with the V4 ICL. Thefourth generation of the Visian ICL (V4, STAAR SurgicalCo., Monrovia, California, USA) has been FDA approvedsince December 2005. After FDA approval, the IOL hadto be named ‘implantable collamer lens’ instead of‘implantable contact lens’. One of the major concerns ofthe ICL was the possible complication of pigment dispersionand secondary glaucoma. However, even few case1 3Phakic intraocular lenses: past and present 277