medtropoleAktuelles aus der Klinik für einweisende Ärzte - Asklepios
medtropoleAktuelles aus der Klinik für einweisende Ärzte - Asklepios
medtropoleAktuelles aus der Klinik für einweisende Ärzte - Asklepios

Sie wollen auch ein ePaper? Erhöhen Sie die Reichweite Ihrer Titel.
YUMPU macht aus Druck-PDFs automatisch weboptimierte ePaper, die Google liebt.
Medtropole | Ausgabe 22 | Juli 2010<br />
Behandlung mit Immunsuppressiva (z. B.<br />
MTX) begonnen werden. [9] Bei beson<strong>der</strong>s<br />
aggressivem Verlauf ist CYC (als Boluso<strong>der</strong><br />
orale Gabe) einzusetzen. Ergebnisse<br />
einer retrospektiven Analyse von 106 ge -<br />
fäßchirurgisch behandelten Patienten mit<br />
Takayasu-Arteriitis zeigen, dass operative<br />
Therapieverfahren additiv zur immun -<br />
suppressiven Therapie die Prognose von<br />
Patienten mit Komplikationen und refraktärem<br />
Verlauf (zum Beispiel bei großen<br />
Aneurysmen) verbessern.<br />
Literatur<br />
[1] Jennette JC, Falk RJ, et al. Nomenclature of systemic<br />
vasculitides. Proposal of an international consensus conference.<br />
Arthritis Rheum. 1994; 37(2): 187-92.<br />
[2] Gross WL. Primäre systemische Vaskulitiden. Teil III.<br />
Pathogenese und Therapie. Der Internist. 1999; 40(11):<br />
1194-215.<br />
[3] Gross WL. Primär systemische Vaskulitiden Teil I:<br />
Allgemeine Übersicht. Der Internist 1999; 40(7): 779-94.<br />
[4] Della Rossa A, Tavoni A, et al. Treatment of chronic<br />
hepatitis C infection with cryoglobulinemia. Curr Opin<br />
Rheumatol. 2002; 14(3): 231-7.<br />
[5] Guillevin L, Cohen P, et al. Treatment of polyarteritis<br />
nodosa and microscopic polyangiitis with poor prognosis<br />
factors: a prospective trial comparing glucocorticoids and<br />
six or twelve cyclophosphamide pulses in sixty-five<br />
patients. Arthritis Rheum. 2003; 49(1): 93-100.<br />
[6] de Groot K, Reinhold-Keller E, et al. Therapy for the<br />
maintenance of remission in sixty-five patients with generalized<br />
Wegener’s granulomatosis. Methotrexate versus<br />
trimethoprim/sulfamethoxazole. Arthritis Rheum. 1996;<br />
39(12): 2052-61.<br />
[7] Fauci AS, Haynes BF, et al. Wegener’s granulomatosis:<br />
prospective clinical and therapeutic experience with 85<br />
patients for 21 years. Ann Intern Med. 1983; 98(1): 76-85.<br />
[8] De Silva M, Hazleman BL. Azathioprine in giant cell<br />
arteritis/polymyalgia rheumatica: a double-blind study.<br />
Ann Rheum Dis. 1986; 45(2): 136-8.<br />
[9] Shikawa K, Maetani S. Long-term outcome for 120<br />
Japanese patients with Takayasu’s disease. Clinical and statistical<br />
analyses of related prognostic factors. Circulation.<br />
1994; 90(4): 1855-60.<br />
814<br />
<strong>Klinik</strong> Substanz<br />
Induktionstherapie<br />
Dosis/Applikation<br />
Cotrimoxazol „Initialphase“ T/S 2 x 960 mg/die p. o.<br />
Methrotrexat<br />
„Fauci-Schema“<br />
blande MTX 0,3 mg/kg/Wo. i. v. o<strong>der</strong> s. c.<br />
NIH-Standard<br />
aktiv<br />
CYC 2 mg/kg die p. o.<br />
intensiviert<br />
progressiv/foudroyant<br />
CYC 3 – 4 mg/kg/ die p. o.<br />
„Austin-Schema“<br />
mäßig-aktiv bzw. überwiegend<br />
renale Vaskulitis<br />
CYC 15 – 20 mg/kg i. v.<br />
Plasmapherese foudroyant mit Nierenversagen 40 – 60 ml/kg (4 – 7x)<br />
Cotrimoxazol Voll-/Teilremission<br />
Erhaltungstherapie<br />
T/S 2 x 960 mg/die p. o.<br />
Methrotexat Teilremission MTX 0,3 mg/kg/Wo i. v.<br />
Azathioprin Teilremission AZA 2 – 3 mg/kg/die p. o.<br />
Cyclosporin A nach Organtransplantation CsA 3 – 5 mg/kg/die p. o.<br />
i. v. Immunglobuline refraktär<br />
Behandlung refraktärer Verläufe<br />
IVIG 400 mg/kg i. v. an 5 Tagen<br />
Monoklonale AK refraktär anti CD4 plus<br />
anti CD52 sequentielle Gabe i.v.<br />
Antithymozytenglobulin refraktär ATG i. v. 10 Tage<br />
Tab. 6: Aktivitäts- und <strong>aus</strong>dehnungsadaptierte Behandlung ANCA-assoziierter Vaskulitiden<br />
Name nach <strong>der</strong><br />
Chapel-Hill Conference 1992<br />
Intensiviertes Protokoll<br />
bei „therapieresistenten“ PSV<br />
Riesenzellarteriitis GC plus AZA o<strong>der</strong> MTX<br />
Takayasu-Arteriitis GC plus MTX<br />
Tab. 7: Behandlung <strong>der</strong> therapieresistenten bzw. -refraktären PSV-intensivierte Therapiemöglichkeiten bei Progression<br />
Kontakt<br />
„therapierefraktären“ PSV<br />
GC puls CYC<br />
(FAUCI- o<strong>der</strong> AustinSchema)<br />
GC plus CYC<br />
(FAUCI- o<strong>der</strong> Austin-Schema)<br />
Polyarteriitis nodosa (PAN) GC & CYC-Bolus plus Plasmapherese GC plus CYC (FAUCI-Schema)<br />
Hepatitis B-Virus-assoz. PAN<br />
IFNα & Lamivudin plus<br />
Plasmapherese<br />
GC plus CYC (FAUCI-Schema)<br />
Wegener’sche Granulomatose<br />
GC & CYC (FAUCI-Schema) plus<br />
IVIG<br />
AK: a-CD4/CD52*<br />
Churg-Str<strong>aus</strong>s-Syndrom GC plus CYC (FAUCI-Schema) α-Interferon (bis 3 x 106/Woche)<br />
Mikroskopische Polyangiitis GC & CYC plus IVIG<br />
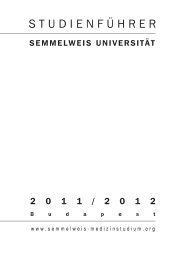
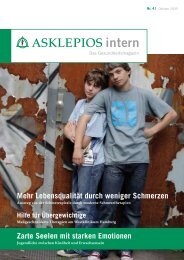
Abb. 1: HRCT-Thorax, Lungengranulom bei M. Wegener Abb. 2: MRT-Kopf, M. Wegener, Mastoiditis<br />
α-Thymozytenglobulin<br />
Monoklonale AK: a-CD4/CD52<br />
Henoch-Schönlein-Purpura GC plus IVIG (evtl. CYC) GC plus CYC (AUSTIN-Schema)<br />
Kutane leukozytoklastische Angiitis GC plus AZA (MTX)<br />
Essentiell kryoglobulinämische α-Interferon & Ribavirin plus AUSTIN-Schema plus<br />
Vaskulitis<br />
Plasmapherese<br />
Plasmapherese<br />
Erläuterungen<br />
GC = Glucocorticoid AZA = Azathioprin „low-dose” MTX = Methotrexat<br />
CYC = Cyclophospamid GC & CP = FAUCI-Schema CP = Cyclophosphamid-bolus = AUSTIN-Schema<br />
* humanisiertes anti-CD4, anti-CAMPATH 1H<br />
Dr. Keihan Ahmadi-Simab<br />
<strong>Klinik</strong> <strong>für</strong> Rheumatologie,<br />
klinische Immunologie, Nephrologie<br />
<strong>Asklepios</strong> <strong>Klinik</strong> Altona<br />
Paul-Ehrlich-Straße 1, 22763 Hamburg<br />
Tel. (0 40) 18 18-81 11 24<br />
Fax (0 40) 18 18-81 48 00<br />
E-Mail: keihan.ahmadi@asklepios.com